I saw this Middle-aged patient with no previous cardiac disease who presented with worrisome substernal chest pain:
 |
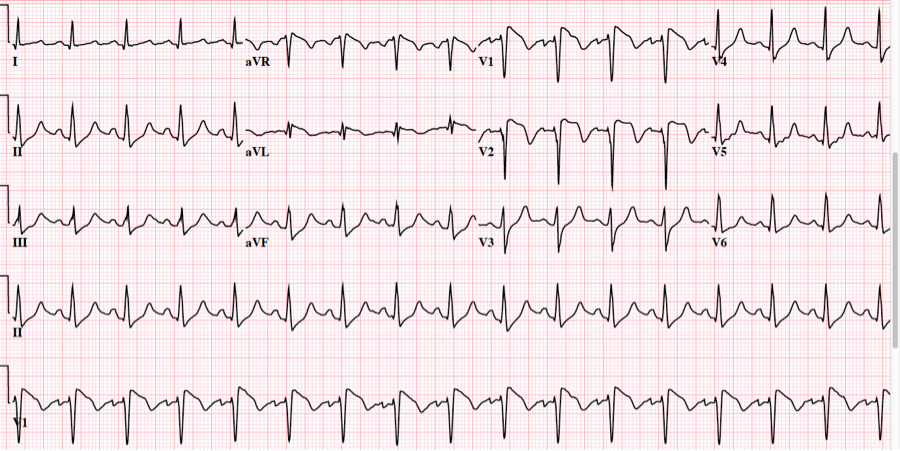
| Sinus rhythm with saddleback ST elevation in V2. There is significant ST elevation here. QTc is 416 ms. There is an upwardly convex ST segment in V3 and V4, which is worrisome. But it really doesn’t look very much like a STEMI, does it? It does not look like early repolarization. There is high voltage (large S-waves and R-waves) and it could all be LVH. Notice there are also prominent U-waves. |
In all my years, I have only reviewed one ECG with a Saddleback ST elevation that was due to STEMI.
Click on this link to see many examples of false positive ST elevation from Saddleback.
A recent previous ECG was available:
 |
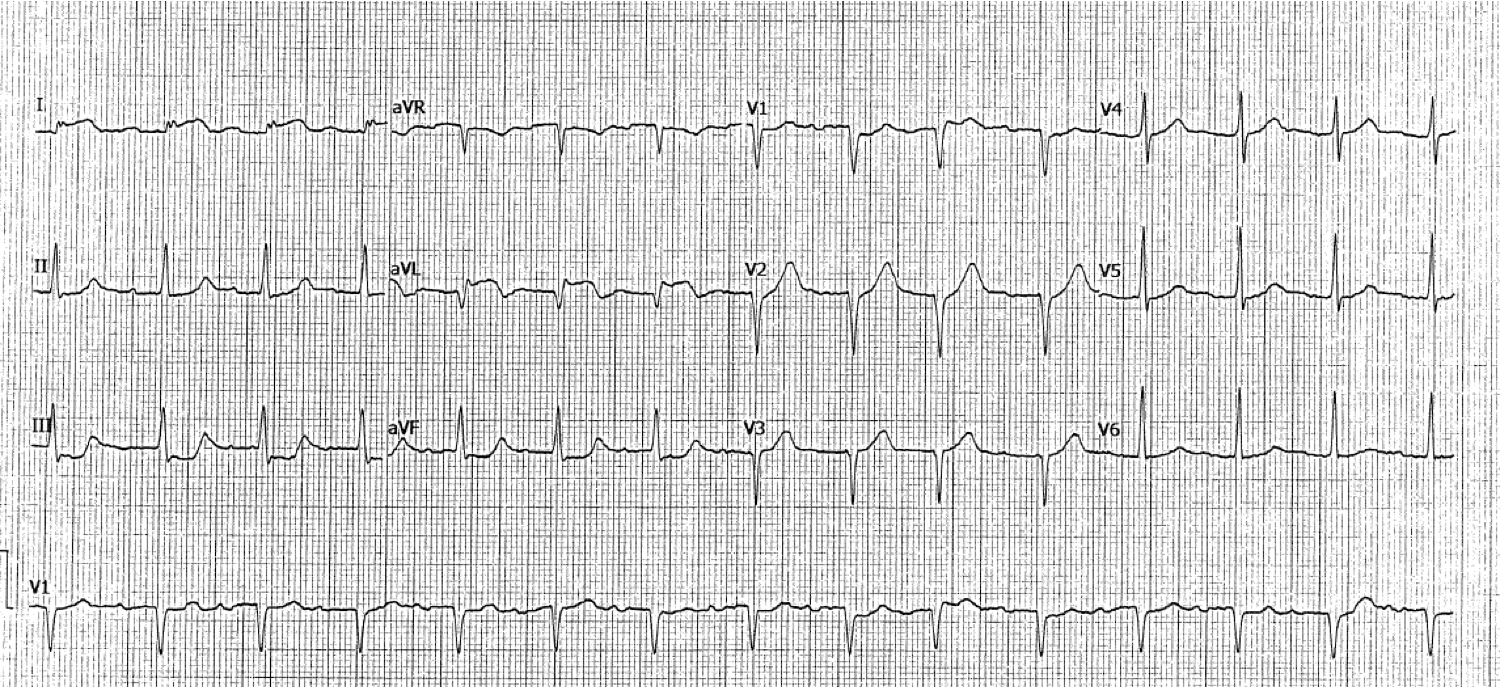
| Looks like early repol except for the Q-wave in V2. QTc is 388 ms. All ST segments are concave upward. |
Here are the precordial leads side by side:
 |
| It still didn’t look like STEMI to me but it was too different to ignore. |
U-waves could be the source of some of the difference, so I checked a K. It was 4.5 mEq/L.
So I activated the cath lab.
While waiting for the cath lab, we did a bedside echo (not shown). We did not see an anterior wall motion abnormality.
I started to get more doubtful.
I ordered a second ECG:
 |
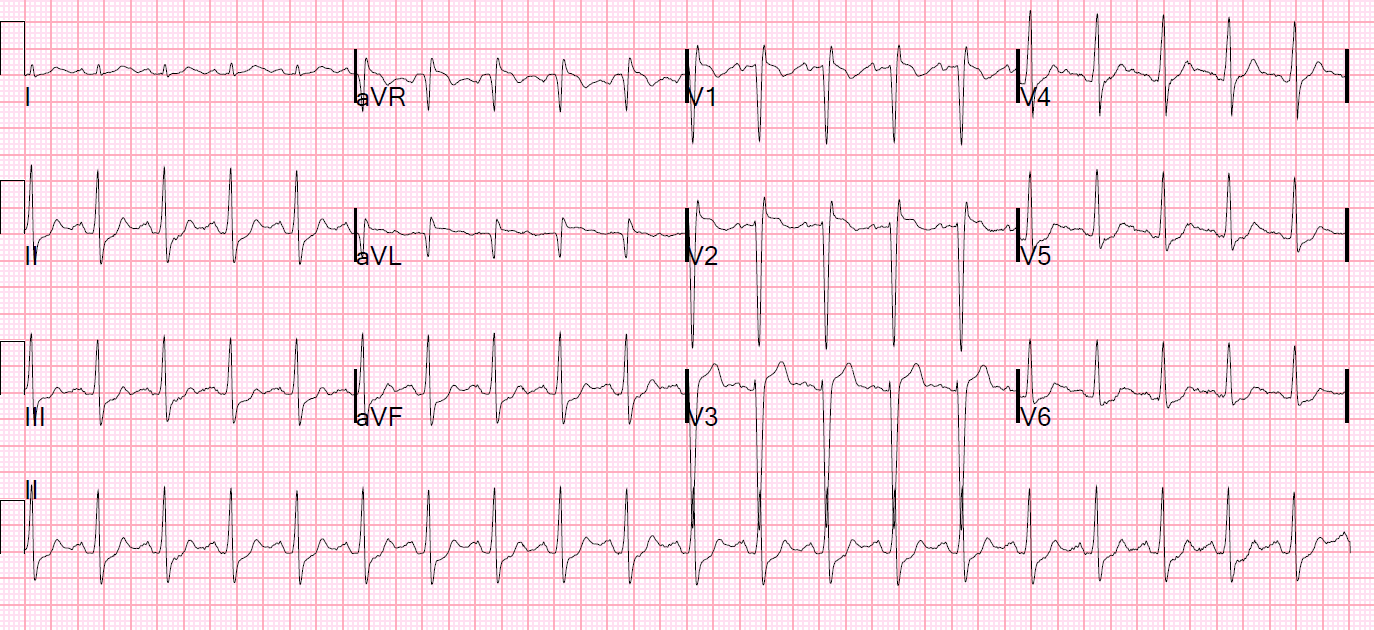
| This looks much more like the old one. There is no saddleback. There is less ST elevation, and less upward concavity |
Knowing that a saddleback can be caused by lead placement too high on the chest (see this paper), I asked the tech if she had changed the lead placement.
She had not.
However, she said she had recorded the first one fully supine. ECGs should be recorded with the patient at a 30-45 degree angle, if possible. (see this reference: http://eprints.ulster.ac.uk/30479/) The second one had been recorded in the 30 degree upright position.
I asked her to record another one with the patient supine:
 |
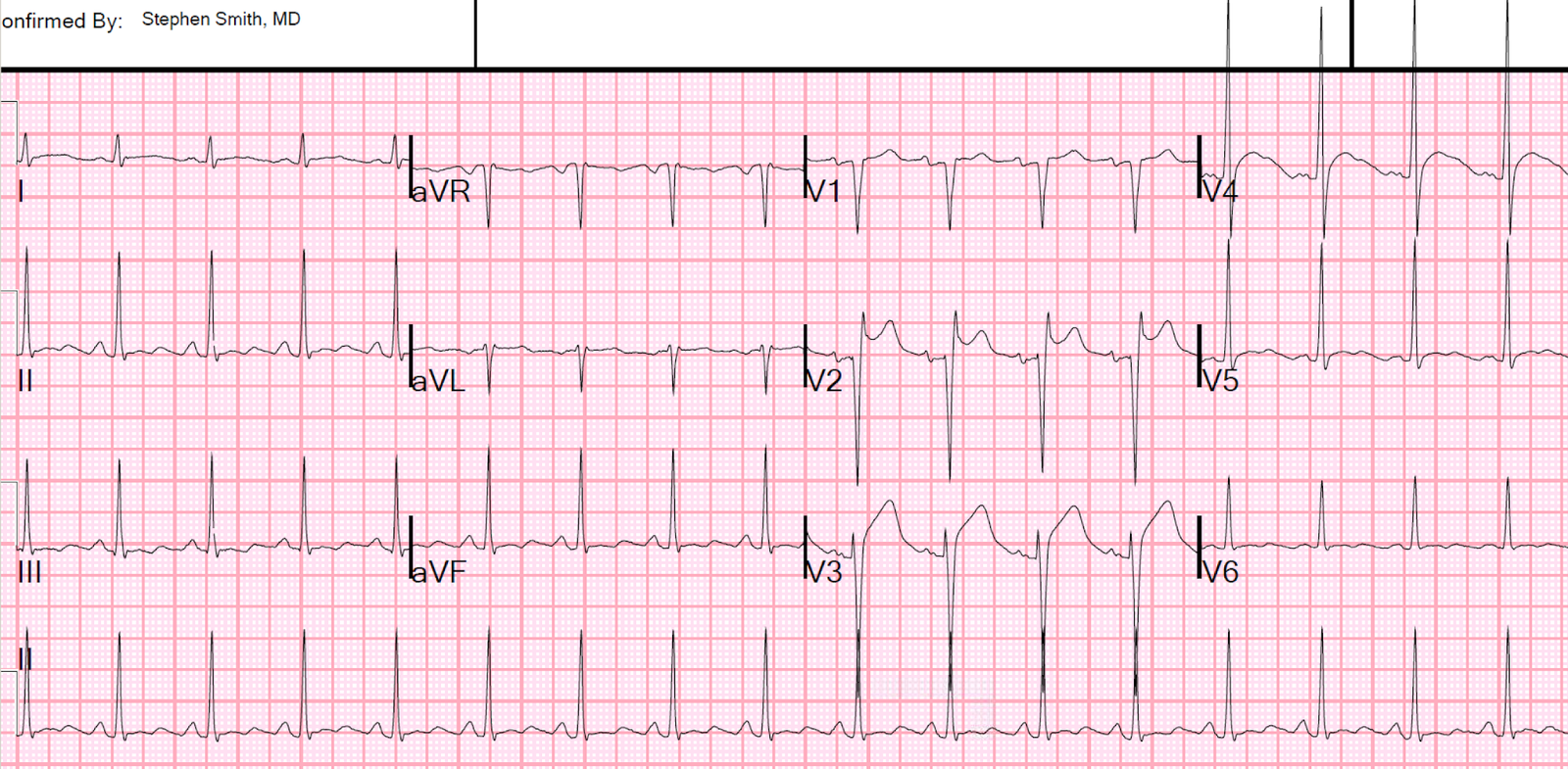
| This again looks a lot like the first one. |
Was this pseudoSTEMI due to artifact due to positioning? Possible, but we do record supine ECGs frequently in patients who are too ill to sit up and they don’t look like this.
Now I was quite certain that this would be a false positive cath lab activation. But it was too late to turn that ship around. The cath team was ready and he underwent an angiogram.
The interventionalist, who was not at all purturbed, said that the coronaries were “huge pipes” and totally clean.
Here is his formal ultrasound result:
Hyperdynamic systolic performance; EF 75-80%.
No regional wall motion abnormality.
Left ventricular hypertrophy-concentric, moderate.
Learning Points:
1. Saddleback ST Elevation is rarely due to STEMI.
2. Make sure the ECG is recorded with good patient and lead position.
3. LVH has a variety of PseudoSTEMI patterns.
4. If there is high precordial QRS voltage, either large S-waves or R-waves, anterior STEMI is unlikely.