And I came across this one while reading EKGs for a high sensitivity troponin study:
 |
| what do you think? |
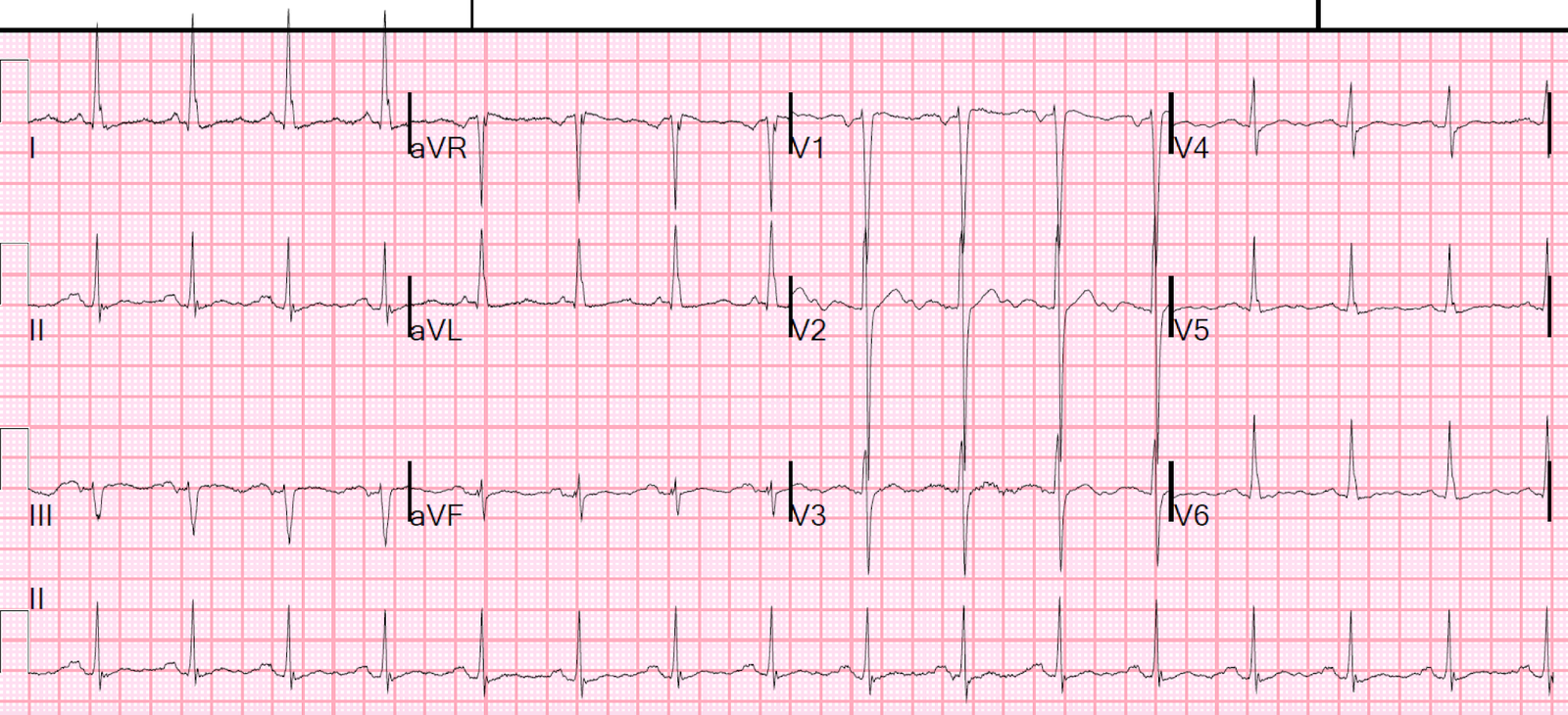
Normally, if one sees STE in aVL with reciprocal STD in III, one would say “Acute OMI”.
But I instantly knew it was not.
I immediately recognized it as normal, and classified it for the study (blinded) as “normal with normal ST Elevation and “normal ST depression.”
All I know when I see the ECG for this study is that the patient has had at least 2 troponins drawn.
I don’t know whether it is for chest pain, weakness, whatever.
I don’t know for certain why my (our) mind immediately knows that it is normal.
I believe it is partly the flat STE, lots of upward concavity in the STE so that T-wave does not look hyperacute (hyperacute T-waves are “fat” because there is less upward concavity).
But there is terminal QRS distortion, which in a large study I just did I found to be quite good for OMI.
The ST axis is barely negative in aVF and slightly positive in II, so it is about -10 degrees, and I’m not sure what to make of that.
I sent it to Ken Grauer and he knew it was not as well.
This is what he wrote:
Hi. I’ll assume “CP” for the history.
- Sinus rhythm. Assuming it’s an adult at least ~35, then the deep S and ST-T wave shape in V2 suggest LVH.
- There is J-point ST elevation in I, aVL. Lead III shows some ST dep with T inversion — but given ONLY seen in lead III (aVF is flat) — I am NOT at all convinced this is necessarily acute!
- I’d want more info, serial tracings, an old ECG, trop, etc — but my hunch is that this is not acute …
- There are U waves (check lytes)
Why do we automatically know it is not ischemic STE/STD?
We are not entirely certain.
It remains an unfortunate fact that some aspects of the ECG are diagnosed by recognition only, like recognizing a face.
This is why I believe AI will be a force for accurate diagnosis of OMI in the future: it is good at recognizing faces, and also ECGs. We have not yet tried to train the Cardiologs Deep Convolutional Neural Network how to recognize OMI, but I hope they will have me do that some day.
After my blinded review, I went to review the case details:
Patient was in his 30’s with acute stroke.
All troponins were undetectable
Echo:
Left ventricular hypertrophy concentric .
The estimated left ventricular ejection fraction is 60 %.
There is no left ventricular wall motion abnormality identified.
![]()
===================================
MY Comment by KEN GRAUER, MD (5/7/2020):
===================================
As per Dr. Smith — both of us immediately suspected the above ECG did not reflect acute changes by its appearance.
- I share the difficulty Dr. Smith expresses in trying to explain WHY my strong hunch was that this was not acute coronary disease.
- I thought the generous R waves as early as lead V2, in conjunction with the deep S wave and ST coving in V2 was most consistent with LVH.
- The shape of the ST elevation in high lateral leads I and aVL is clearly upward coving — which often signals a benign repolarization change.
- The main abnormal finding was that ST-T depression in lead III — but in isolation (ie, with a perfectly normal ST-T wave in lead II — and no more than a flat ST segment in lead aVF) — I didn’t think this was necessarily abnormal (especially given the unusual rSr’ QRS morphology pattern in lead III, in which there is predominant negativity in lead III, that is so often naturally accompanied by T wave inversion, simply because the T wave vector tends to follow closely behind the QRS vector, and that is predominantly negative in lead III … ).
A major part of my ECG interpretation experience came from being the sole interpreter of all ambulatory tracings ordered by 35 providers in a primary care clinic over a 30-year period. I often was not given any history for the multiple tracings I had to interpret.
- This type of ECG would be among the ~5% of tracings for which I would say to myself — “I don’t think this ECG represents acute coronary disease — but since I’m not 100% certain, I will immediately stop what I’m doing to go pull the chart (and/or call the provider) to get more history (and look to see if there is a prior tracing) — so that I can be more certain that what I’m seeing on the ECG is not an acute change.
- BOTTOM LINE: It is often difficult to be 100% certain. Being ~90% certain (as I was after seeing this tracing) — is not “good enough” if there is a 5-10% chance that I might overlook something acute. The GOOD NEWS (as Dr. Smith has illustrated numerous times on this Blog) — is that additional measures (ie, clinical follow-up over ensuing minutes of the patient, serial ECGs, looking for a prior tracing for comparison, stat Echo during symptoms, troponin, etc) will usually allow the emergency provider to get much closer to that 99% certainty level about the patient.
![]()