A completely healthy 39 year old woman with no cardiac risk factors had sudden onset of bilateral trapezius pain that radiated around to her throat. It resolved after about 5 minutes, but then recurred and was sustained for over an hour. She called 911.
EMS recorded these ECGs:
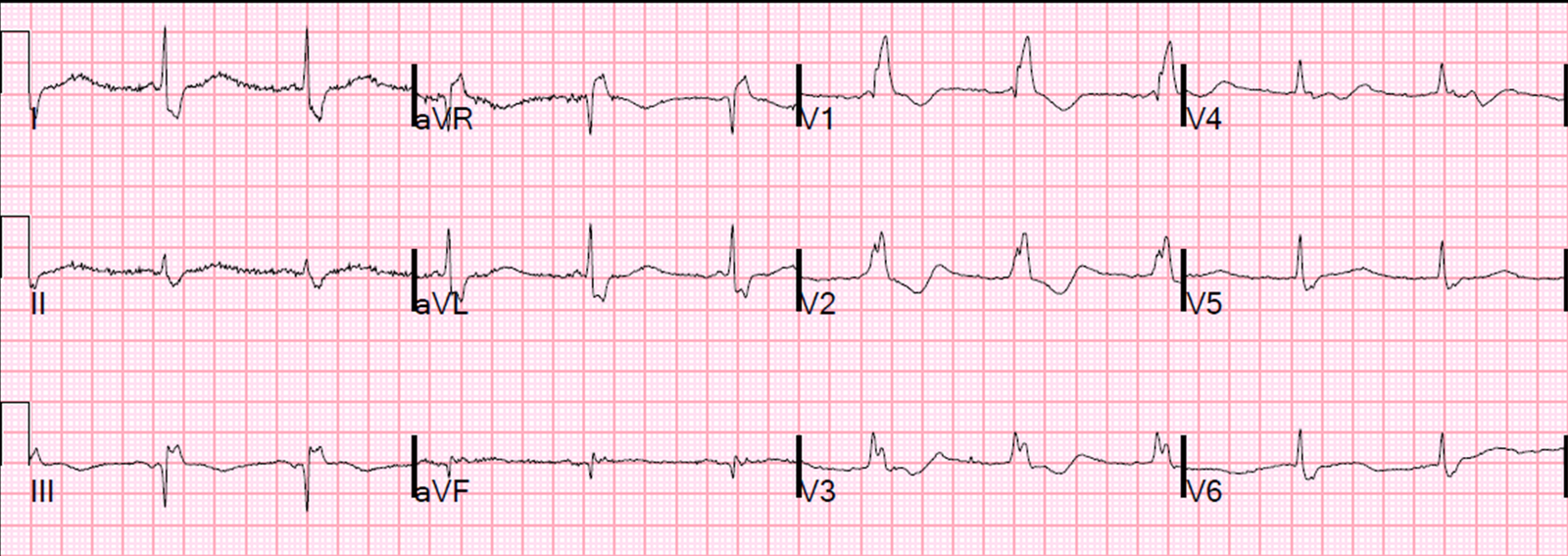
Time 0:
 |
| In V2-V4, there is ST elevation that does not meet STEMI “criteria,” of 1.5 mm at the J-point, relative to the PQ junction. But there are also unusually Large T-waves |
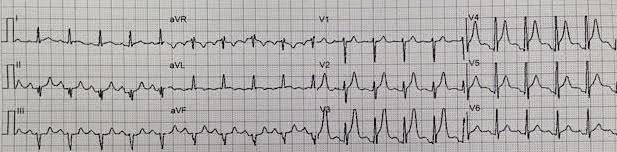
Time = 13 min
 |
| T-wave in V2 is now taller and fatter, the ST segment is more straight. T-wave in V3 is no taller, but it is fatter due to a straighter ST segment This is highly suspicious for early LAD occlusion |
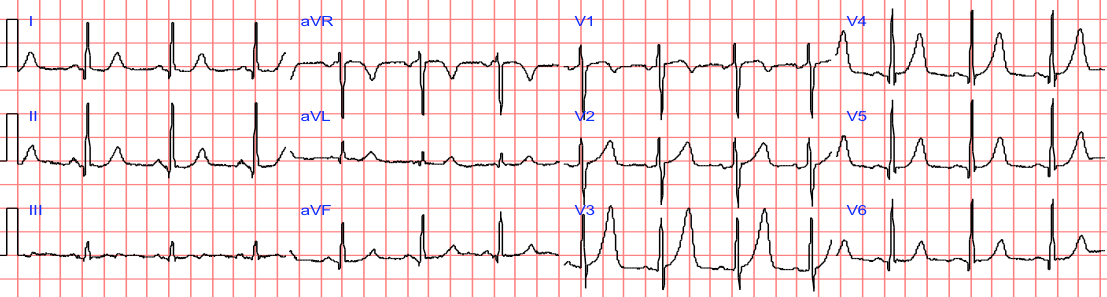
Time = 24 min
 |
| No significant change |
Time = 25 min
These prehospital ECGs were lost and not seen.
The patient arrived in the ED.
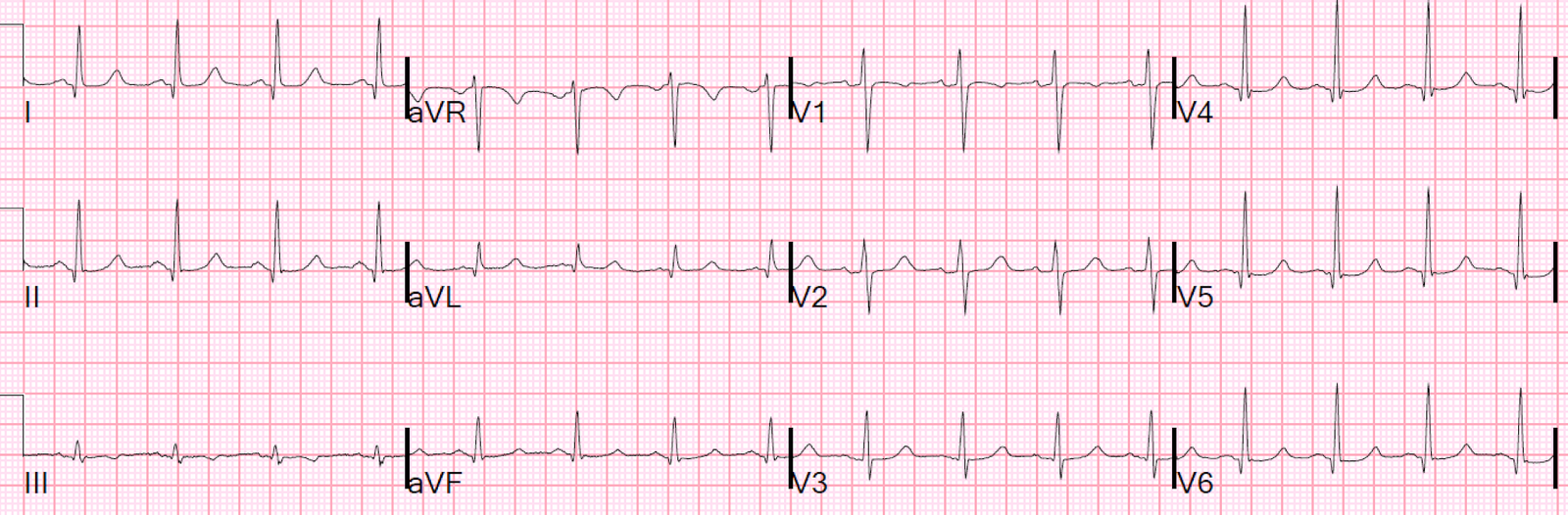
The pain completely resolved after nitroglycerine, and just before this ECG was recorded in the ED (she had been pain free for moments only when this was recorded):
 |
|
Computer read: Normal ECG. The T-wave in V2 is smaller, but so is the QRS; so the proportion is not different. |
This patient has a nondiagnostic ECG by most rules. However, with attention to subtleties, it is very worrisome.
If you use something like the HEART score:
1. H History: She has atypical pain (trapezius) (score = 0-1, depending on the physician)
2. E EKG: a negative ECG (score = 0 or 1, most would say 0)
3. A Age: = 0
4. R Risk factors = 0
5. T: Troponin = 0 [first troponin (contemporary, not high sensitivity) was less than the level of detection).
Total HEART score = 0-2. Risk of 30-day adverse events is less than 1.7%. Some might send her home.
But maybe she has an acute LAD occlusion that will get even worse.
The providers did a bedside echo and even used speckle tracking to look for strain:
I think maybe there is an anterior wall motion abnormality, but this is very difficult. They read it as normal.
Here are a couple shots with strain, or “speckle tracking” on ED Echo:
To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this.
She said:
This is a tough one. I see what you mean, initially when I looked at the
image, I also thought there was an anterior wall motion abnormality. But then on closer inspection, I suspect that
maybe the anterior wall is just not being tracked well. In systole, you
can see the anterior wall come down and outside of the area that is
being tracked (more so than the other tracked walls). Even though the
strain values are a little off in the graph (so is the posterior wall)
it is still a value range (about -18) that would be considered
non-ischemic by the cardiology literature, I believe. I have been wrong
before though! So it is possible that I am misinterpreting the clip. If
it were me, I would get values at the level of the mitral valve,
papillary muscles, and apex (all in PSS axis). Also, narrowing the area
being tracked helps the walls get recognized much better.
As I wrote, the first troponin was below the Level of Detection.
She remained pain free, and was admitted without further serial ECGs.
When in doubt, one should always get serial ECGs. Bedside echo is not enough.
At time = 240 minutes (4 hours), the second troponin returned at 1.15 ng/mL. That prompted recording of this ECG:
 |
| Back to normal for this patient. This demonstrates that all ST elevation of the previous ECGs was ischemic, not normal. She was having a transient STEMI, briefly. |
It is very lucky that she spontaneously reperfused her LAD. It did not progress to full STEMI with loss of the anterior wall, as in this case.
Also, persistence of a pain free state does not guarantee an open artery. See this case.
A formal contrast echo was done at this point:
Normal estimated left ventricular ejection fraction, 65%.
Regional wall motion abnormality-distal septum and apex.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. It was stented.
Learning Points:
1. Always get serial ECGs when there is any doubt about what is going on.
2. Always find and look at prehospital ECGs. They give extremely valuable information.
3. Hyperacute T-waves remain for some time after reperfusion of an artery. I always say that “you get hyperacute T-waves both ‘on the way up’ (before ST segment elevation) and ‘on the way down’ (as ST elevation is resolving).
4. Wall motion abnormalities are very hard to see, even with advanced Speckle Tracking technology. They require a great contrast exam and expert interpretation.
5. This case does not demonstrate it, but a wall motion abnormality may disappear after spontaneous reperfusion (see this case).
6. Patients with transient occlusion may manifest only transient STEMI on ECG. Subseqent troponins may be all negative and subsequent formal echo may be normal. See this case.