A patient with was resuscitated from respiratory and cardiac arrest of uncertain etiology, but because she was very difficult to ventilate with BVM ventilation, and there were no ultrasonographic slidings signs, pneumothorax was suspected and bilateral needle thoracostomies were placed. This ECG was recorded:
 |
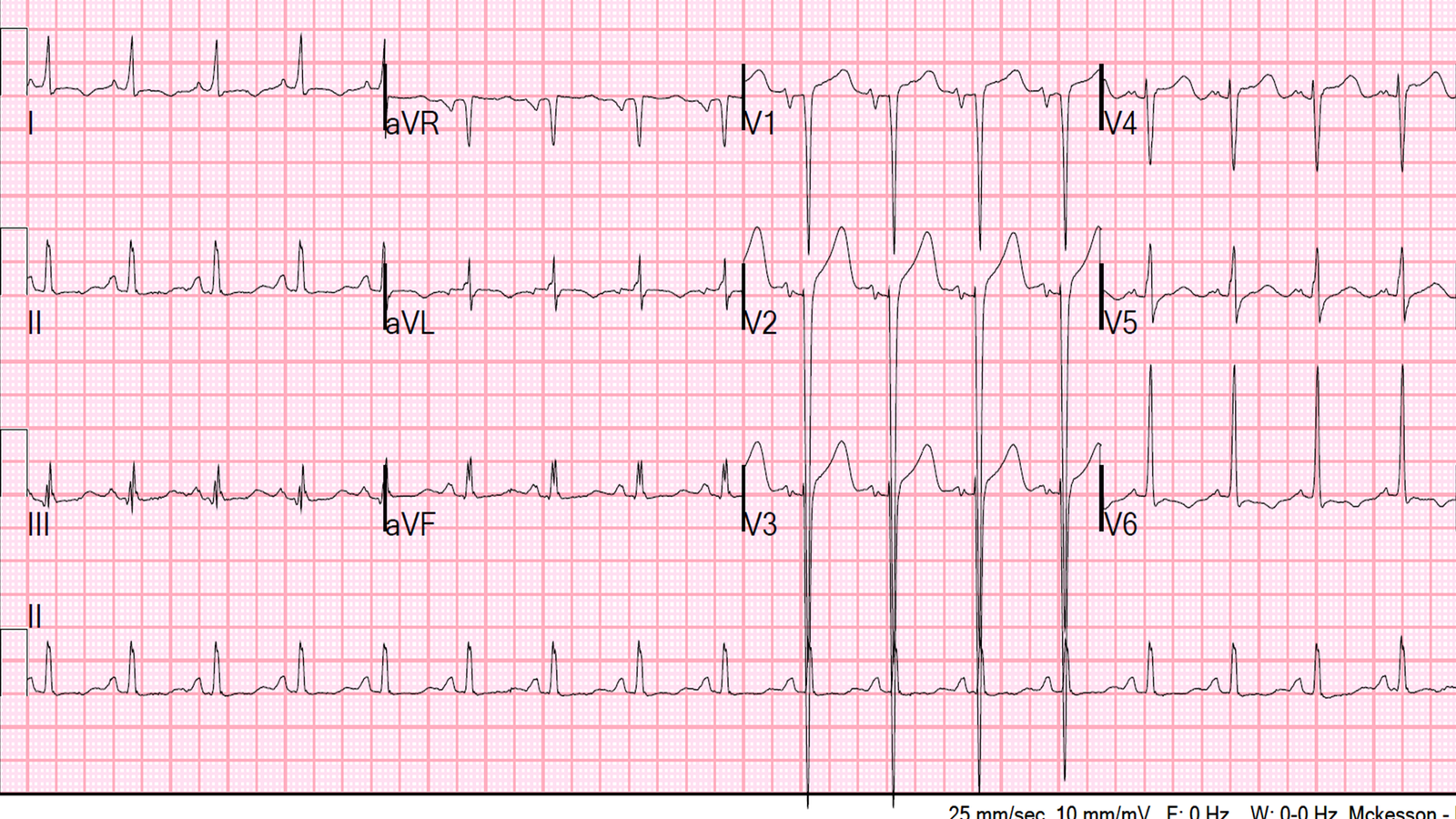
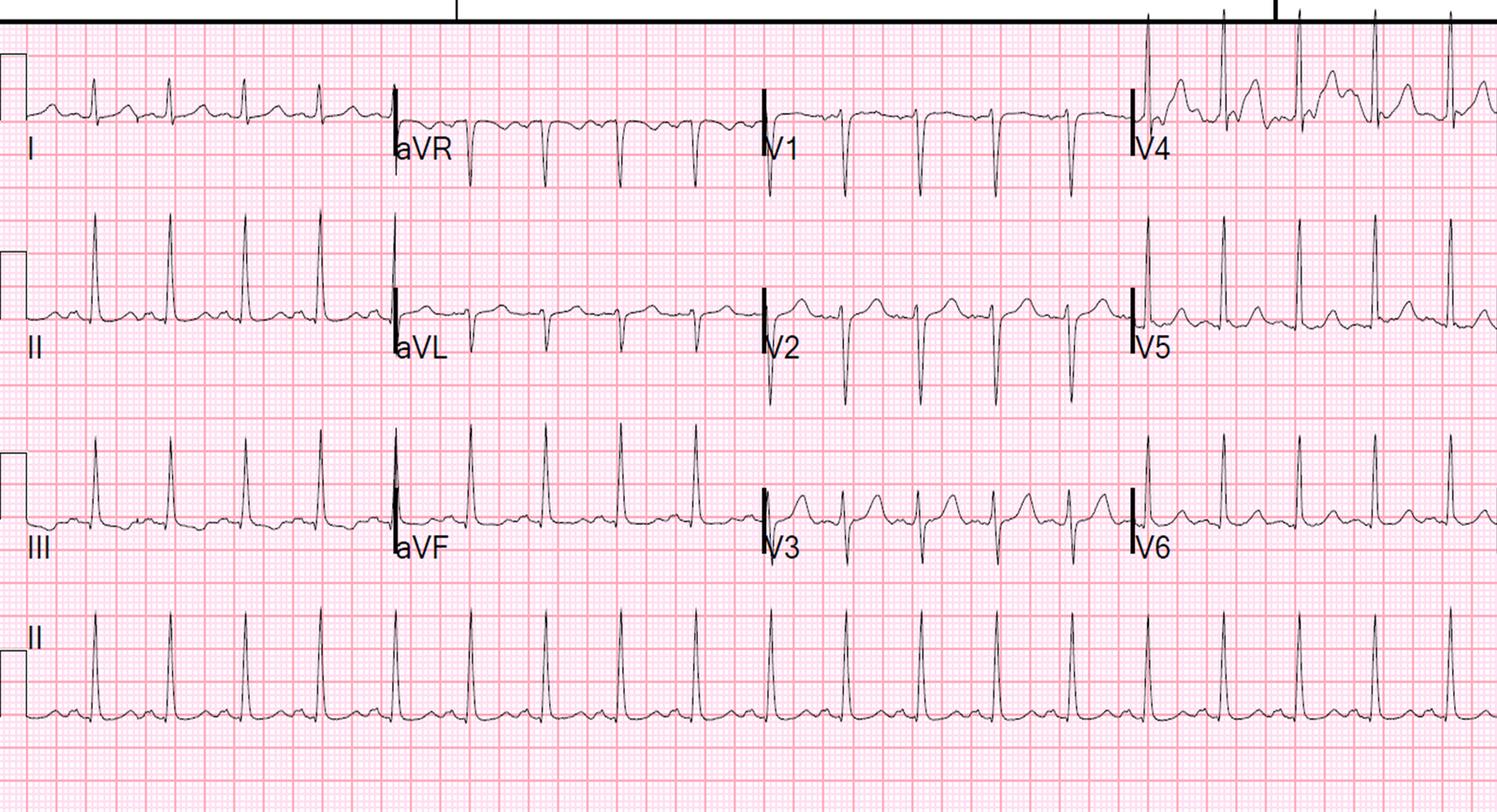
| There is sinus tach and very low voltage in the precordial leads. It is otherwise unremarkable, especially for a patient who was in cardiac arrest. |
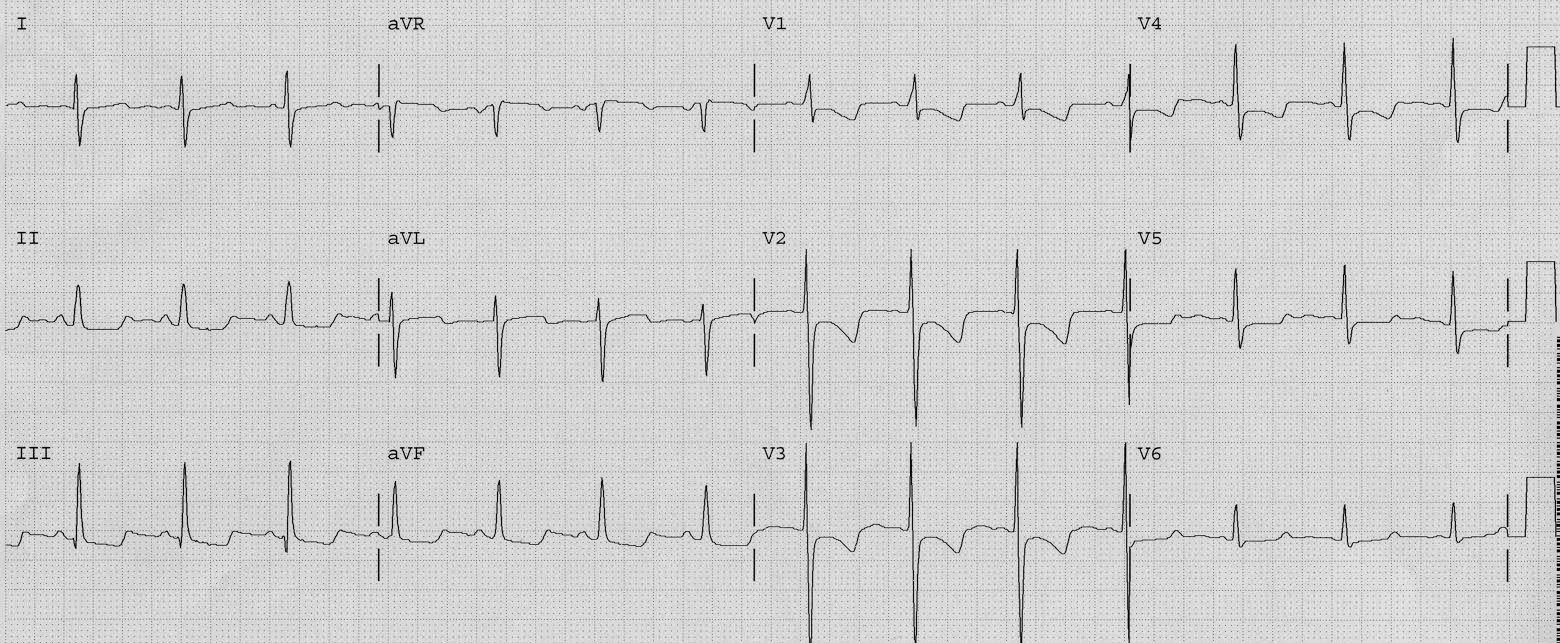
There was a previous ECG available:
 |
| The low voltage is indeed new, and there is no change in limb lead voltage |
Why is there low voltage?
Although she was thought to probably have severe asthma, she underwent a CT pulmonary angiogram to rule out pulmonary embolism. Here it is:
 |
| Air surrounds the heart (pneumopericardium and pneumothorax) |
The air explains the low voltage, but why is the voltage not diminished in the limb leads?
(I don’t know the answer, and I’ll add that the CT scan showed air surrounding the entire heart, in all planes.)
The QRS is said to be low voltage when:
- The amplitudes of all the QRS complexes in limb leads are less than 5 mm; or
- The amplitudes of all the QRS complexes in precordial leads are less than 10 mm
There are several etiologies of low voltage:
- Obesity
- Emphysema
- Pericardial effusion, Pleural Effusion
- Severe hypothyroidism (myxedema)
- Subcutaneous emphysema
- Pneumothorax or Pneumopericardium
- Old large MI
- End-stage dilated cardiomyopathy
- Infiltrative/restrictive diseases such as amyloidosis or hemochromatosis.