This was sent by Michael Macias (Twitter: @EMedCurious), a 4th year EM resident at Northwestern in Chicago.
Case:
An elderly man with end stage renal disease and coronary disease presented with chest pain.
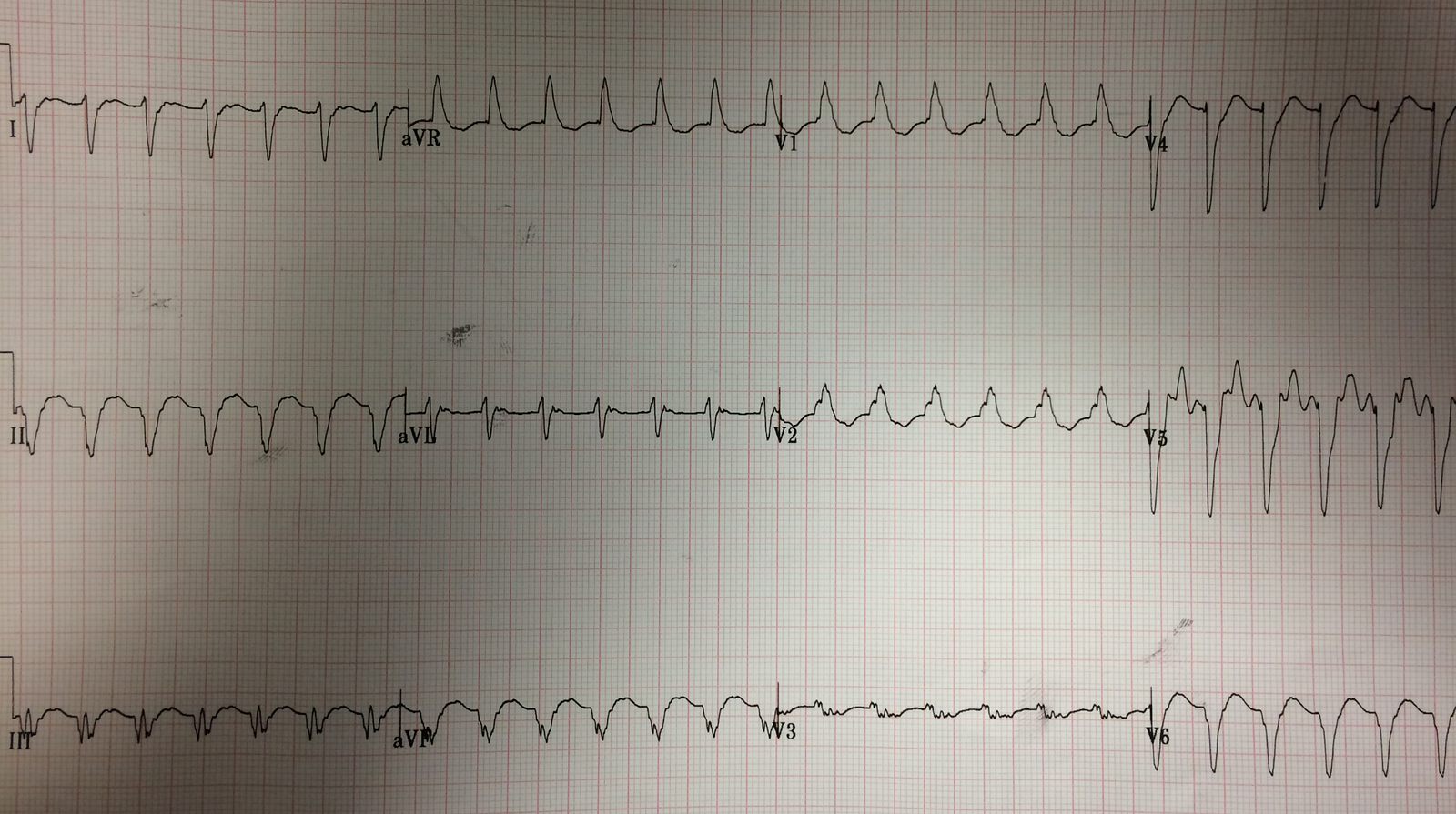
Here is his ECG:
 |
| See the computer interpretation above. What do you think? |
Dr. Macias’ interpretation is here:
Significant elevation in aVR with diffuse ST depression. Hemoglobin was 7.0 g/dL. I thought this was likely triple vessel disease with subendocardial ischemia, but we activated the cath lab given impressive ECG and his history.
Smith interpretation:
The computer reads LVH with repolarization abnormality. There is high voltage, and you expect some discordant ST depression, but this ST depression, although always discordant, is way out of proportion to the QRS voltage. Moreover, the ST depression is NOT maximal in V5 and V6, as it should be with LVH repolarization abnormalities.
So this is ischemic ST depression.
Whether it is diffuse subendocardial ischemia or posterior STEMI is more problematic.
As the STE is most profound in V3 and V4, NOT V5 and V6, posterior STEMI is more likely. However, the STE in aVR (which is reciprocal STE, reciprocal to the ST depression vector towards the apex), is more typically seen in diffuse subendocardial ischemia. ST depression due to subendocardial ischemia is most commonly caused by demand ischemia. One cause of demand ischemia is severe anemia, but a Hgb of 7.0 does not qualify, especially without any tachycardia.
So this must be assumed to be due to ACS.
In fact, the ST depression in V5 and V6 is not all due to ischemia: it is a combination of LVH repolarization and ischemia; the ischemia component is only one portion and so there is less ischemic STD here than one might at first think. This means that the ischemic ST depression is significantly more profound in V3 and V4.
So this is most likely a posterior STEMI pattern, superimposed on LVH. Activating the cath lab is indicated!
Outcome:
100% acute circumflex occlusion, opened.
Learning Points:
1. Again, the computer algorithm cannot be trusted.
2. Posterior STEMI has more ST Depression in V3 and V4. Subendocardial ischemia is maximal in V5 and V6.
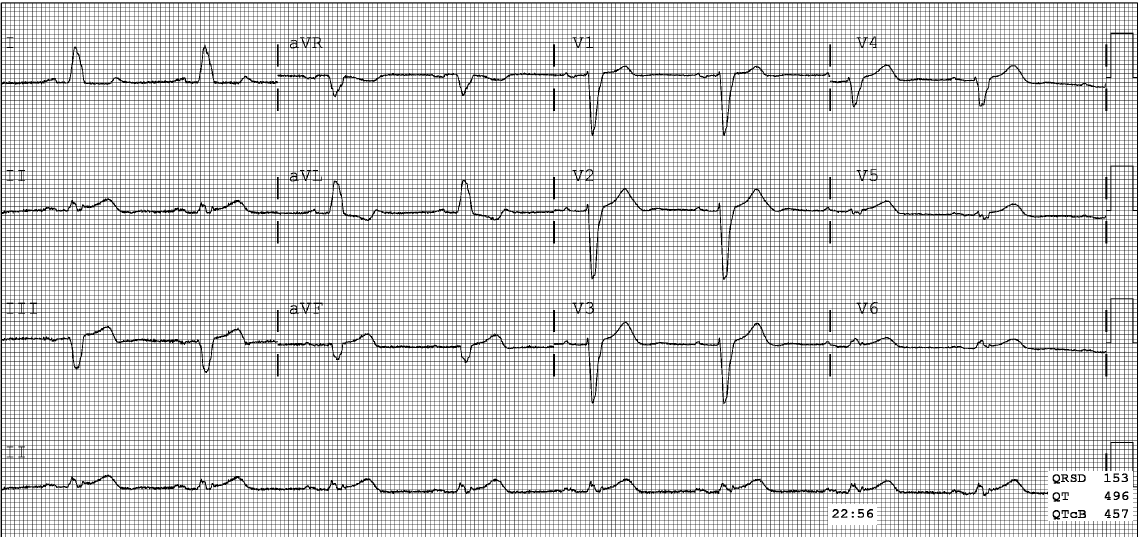
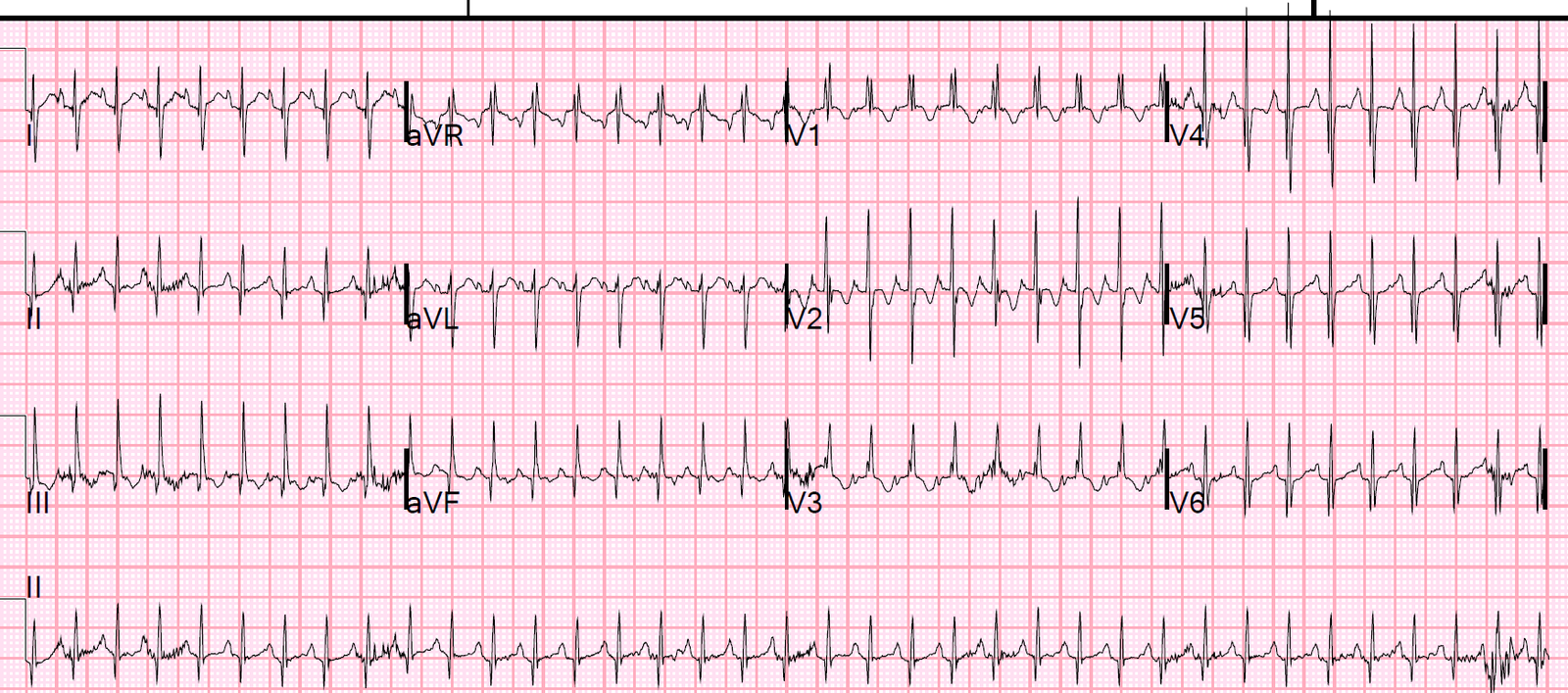
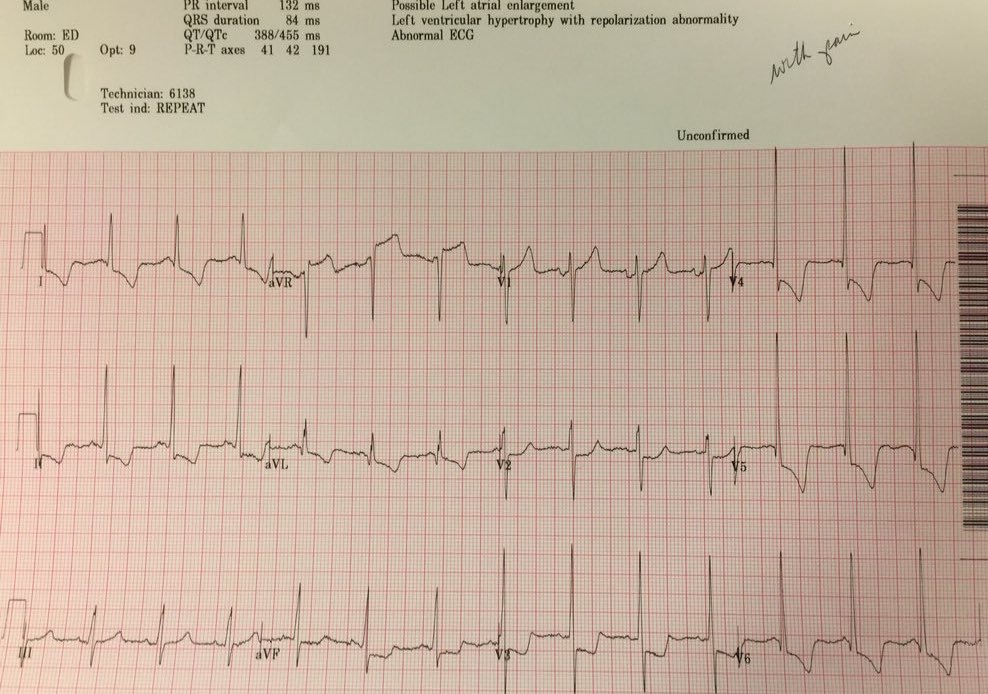
3. Know the expected amount of repolarization abnormality in the presence of LVH. I don’t have a calculated ratio. Below are two examples of LVH with repolarization abnormalities. These are both baseline ECGs without any active ischemia. Notice the proportional amount of ST depression, and that it is maximal in V5 and V6.