This middle-aged male with history of 3 previous stents, 2 in the RCA, had Syncope, Diaphoresis, Nausea, and Dizziness.
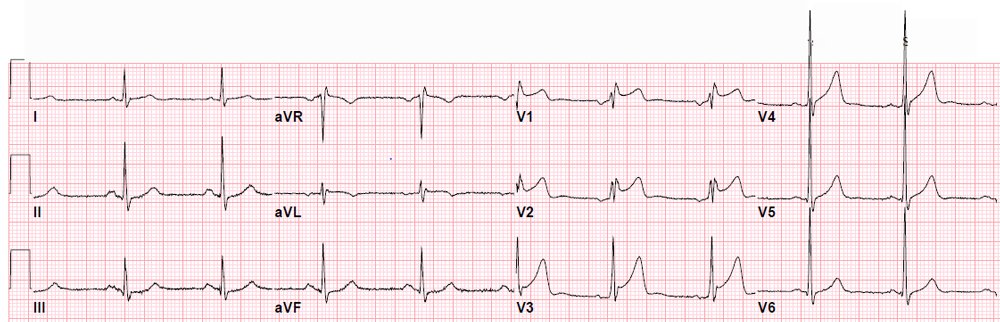
He called 911 and the medics recorded an ECG that looks just like his first ED ECG:
 |
| There is inferior ST elevation and reciprocal ST depression in I and aVL, with reciprocal T-wave inversion in I and aVL. |
This ECG was texted to me (while out on a beautiful point on an island!) with the question: “Would you activate the cath lab?”
I responded: “Yes or at least get stat echo. It is 90% certain to be occlusion.”
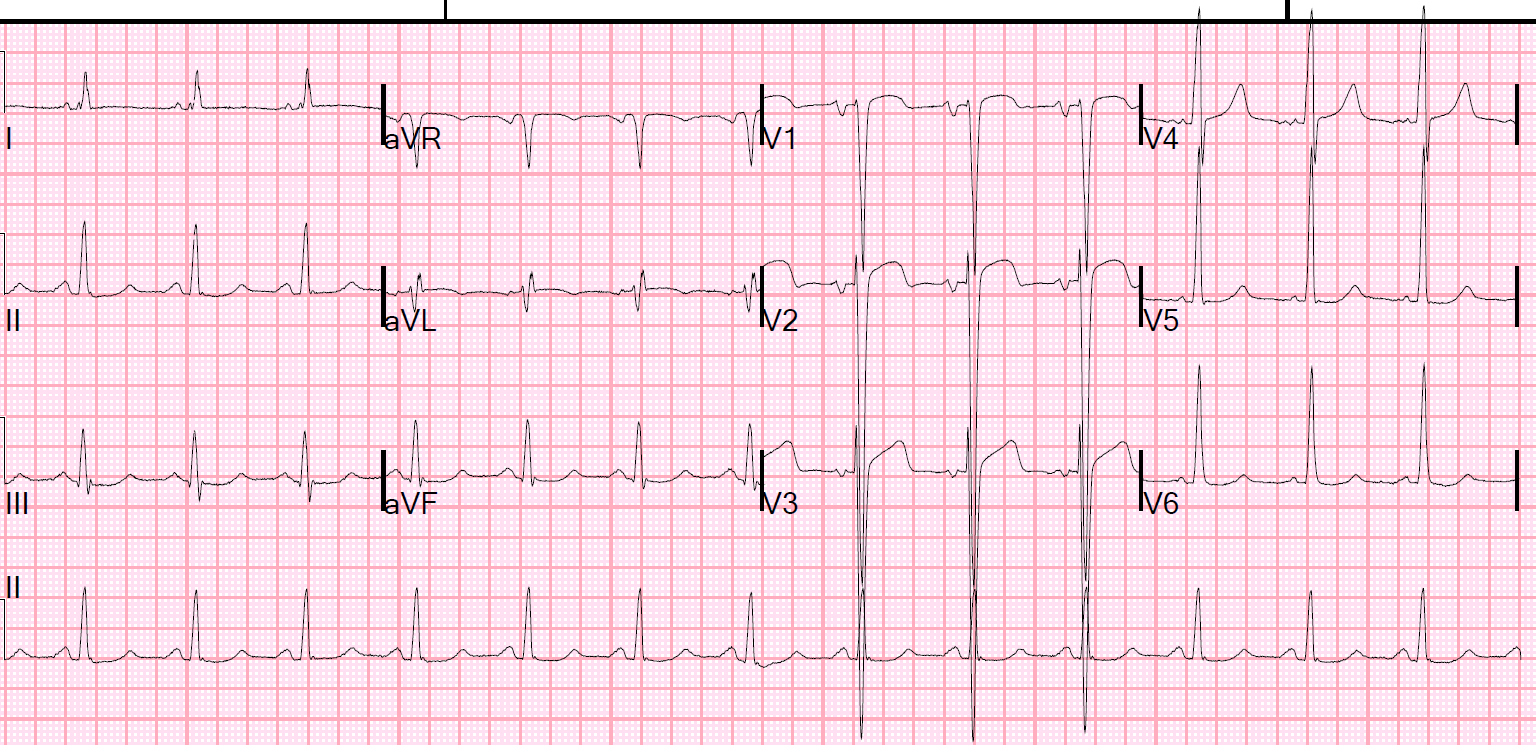
Outcome: The coronaries were clean. The troponins were negative. The subsequent ECGs did not evolve (this latter is the best evidence that there was no MI, as transient ACS can have all of the following negative: Cath, troponins, and Echo).
It turns out that the patient had a similar false positive activation 1/2 year ago because this is his baseline ECG.
He must carry a copy with him wherever he goes!!
Sometimes you just have to have a false positive. You must activate anyway. You cannot let an ECG like this go without action unless you know it is the baseline.
If there is any doubt, it would be reasonable to find an old EKG and/or to get an emergent echo.
Pretest probability: This also points out (again) that when patients do not have chest pain, especially if they do not at least have dyspnea, the probability that their ECG represents a STEMI decreases considerably.