This patient presented with a sudden right sided weakness and ophthalmoplegia that was resolving upon presentation to the ED.
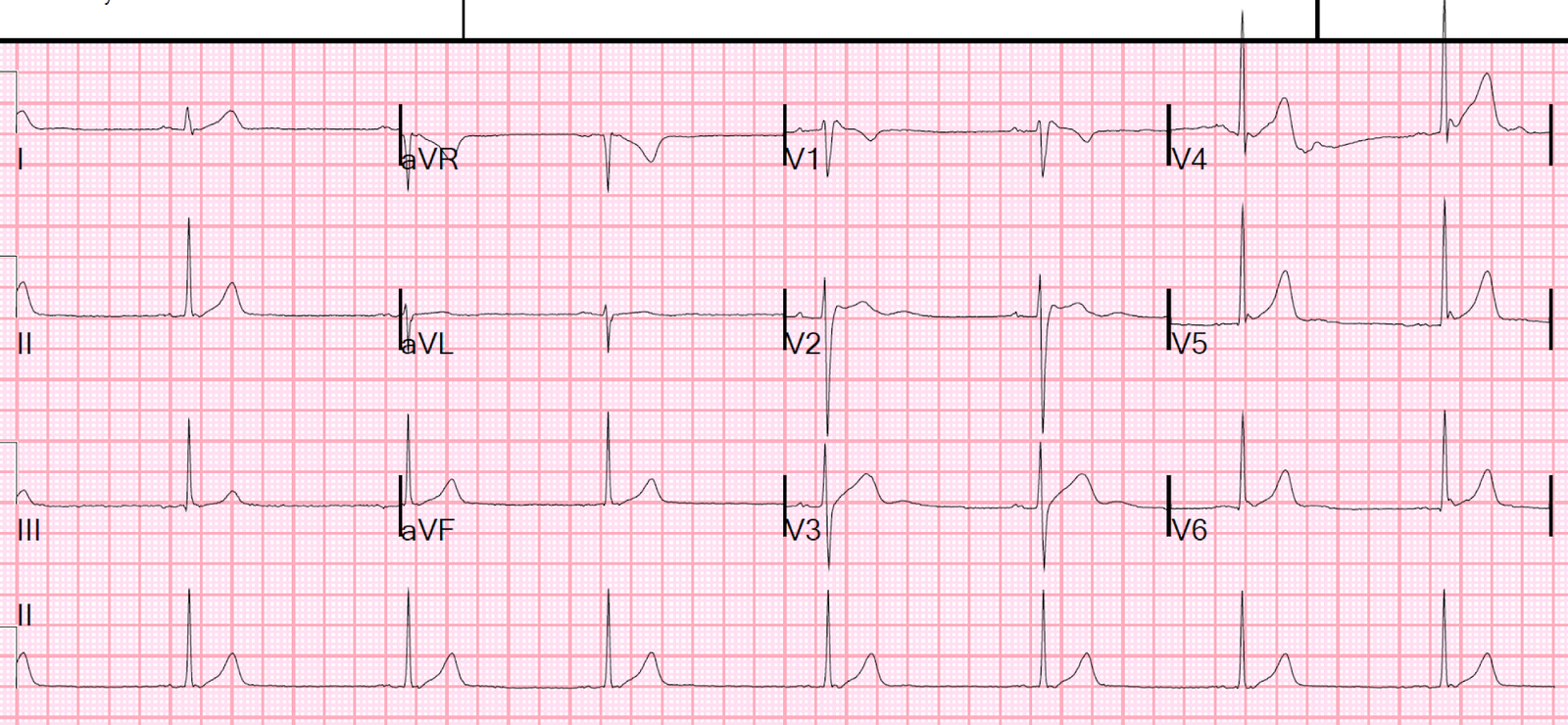
Here is his ED ECG:
 |
| What do you see? |
There are anterior Q-waves, and even some ST elevation. This is suggestive of LV aneurysm. CT and CT angiogram were normal. As all symptoms were resolved, no intervention was undertaken.
MRI confirmed small strokes and some atherosclerotic cerebrovascular disease, which could have been the source of the stroke.
However, because of the ECG findings, an echocardiogram was done which confirmed LV aneurysm and showed:
1. Decreased left ventricular systolic performance moderate to moderately severe
2. Estimated left ventricular ejection fraction of 35%.
3. Regional wall motion abnormality distal anterior wall and apex diastolic distortion with dyskinesis (aneurysm).
4. A 1.2 x 1.3 cm mural thrombus, the source of embolism causing the patient’s TIA.
LV aneurysm is a common substrate for LV thrombus. Whenever you see possible LV aneurysm on the ECG, you should suspect an LV thrombus.
The patient was started on heparin and transitioned to coumadin. He could not recall ever having a myocardial infarction.
Learning Point:
The ECG can be helpful in finding an embolic source of stroke if:
1. There is atrial fibrillation
2. There is evidence of LV Aneurysm, which may harbor a thrombus as source of emboli