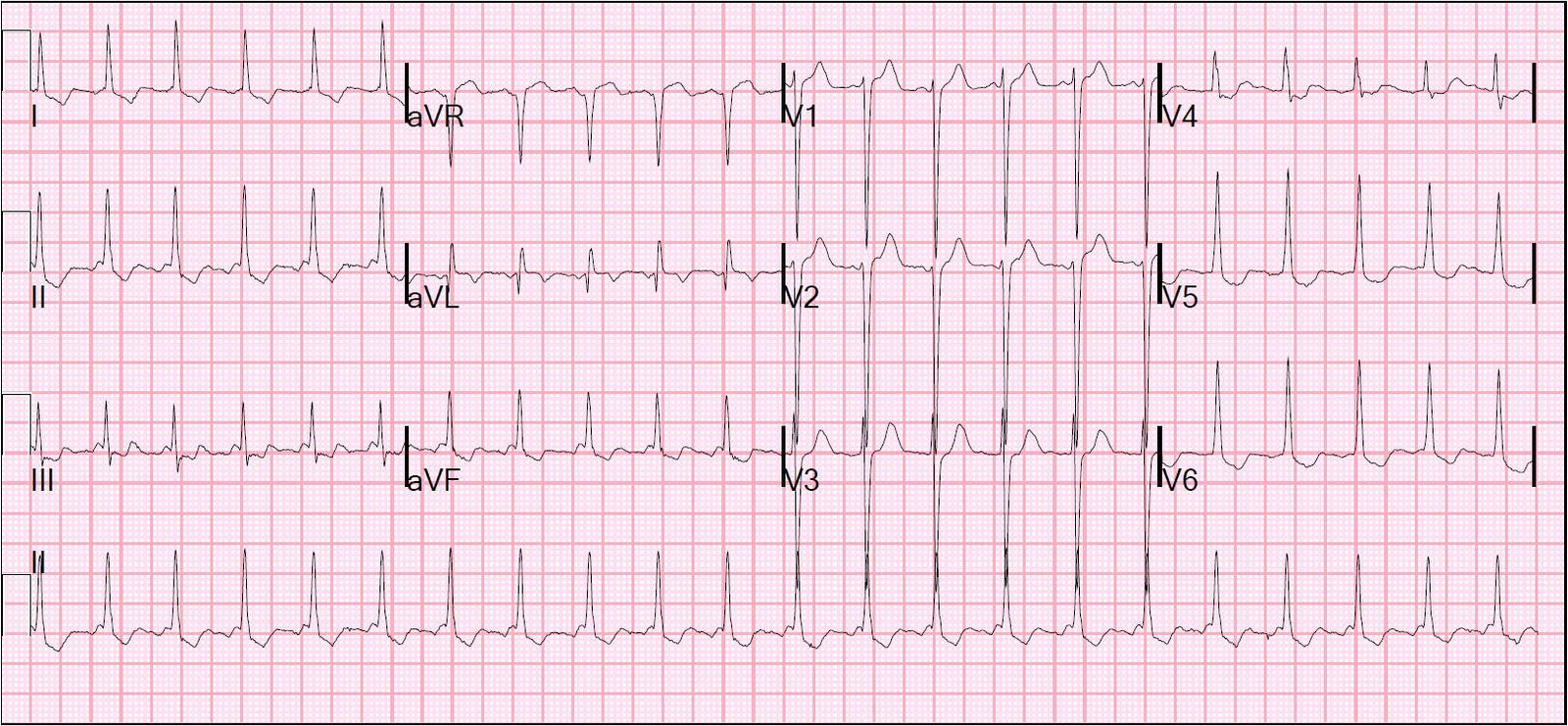
Case 1. Temperature 30 degrees Celsius (86 degrees F) due to environmental hypothermia.
 |
| There is very slow atrial flutter (rate = 167) with 4:1 AV conduction. There is a wide QRS with a very large notch (in this case, a hump), or J-wave, at the end. This is the classic Osborn wave of hypothermia. |
click on ECGs for better resolution
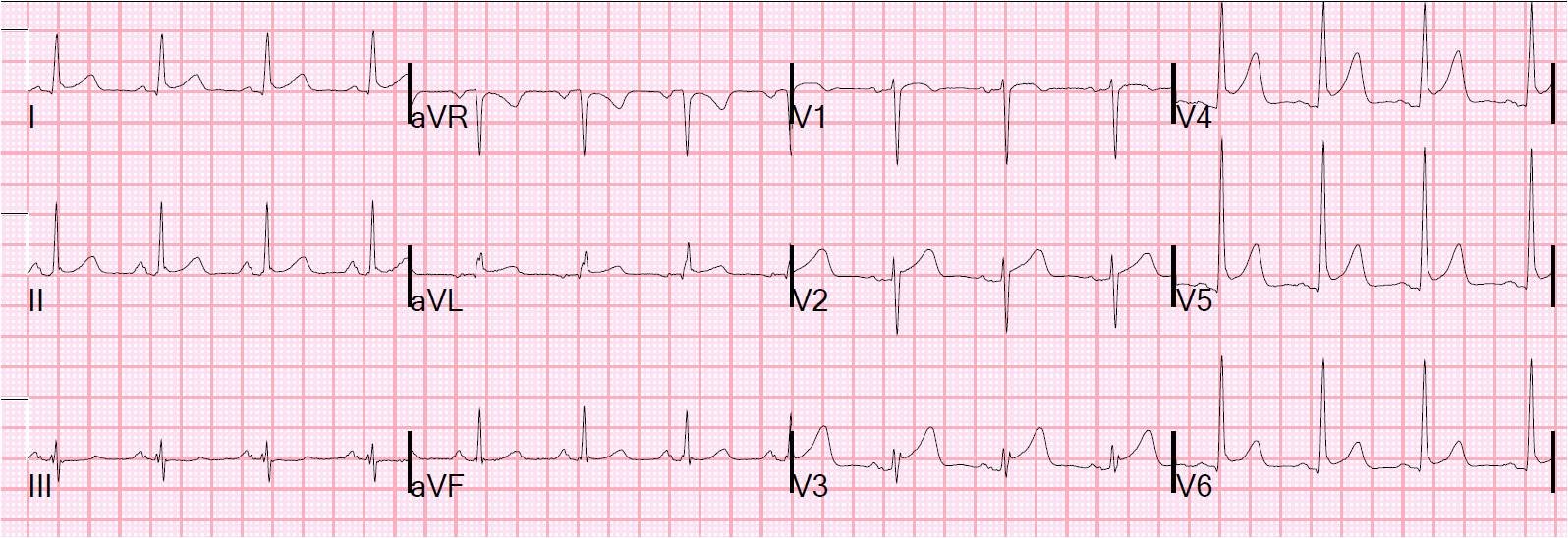
Case 2. A young paraplegic presented confused. Among the early tests performed was this ECG which was showed to me:
 |
| Sinus rhythm. Long QTc [about 500ms; the computer read 180ms (!)]. There is ST elevation which alarmed the residents. I did not think it looked like injury. There are J-wave notches at the end of the QRS, particularly in V3, which are rather large for early repolarization, which should make one think they may be Osborn waves. |
I asked about the temperature.
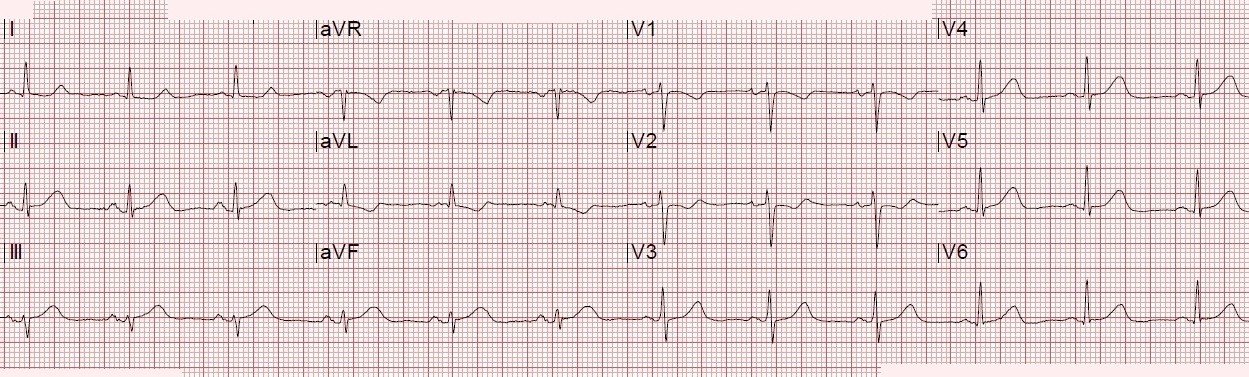
Here is the patient’s previous ECG:
 |
| No ST elevation, and much smaller J-wave notching, seen best in V4. |
A rectal temperature was 30.8 degrees Celsius.
Here is the ECG after rewarming:
 |
| J-wave notching persists but is much smaller. |
Here they are side by side to better see the difference:
 |
| The J-waves are subtly larger in the hypothermic condition |
The ECG in hypothermia
Rhythm: The most common rhythms in hypothermia are sinus bradycardia, junctional bradycardia, and atrial fibrillation. Shivering artifact is common. Atrial flutter is seen in case 1. At temperatures below 30 C, the patient is at risk for ventricular fibrillation. In this study of 29 humans cooled to 28-30 C for cardiac surgery, 19 developed atrial fibrillation and 2 ventricular fibrillation.
QRS: Osborn waves are thought to be pathognomonic of hypothermia, but can also be seen in normothermic patients. “J-waves” or “J-point notching” is very common in early repolarization. Very narrow Osborn waves were reported in severe hypercalcemia (level 16.3). Sometimes a short ST segment of hyperCa can be misinterpreted as an Osborn wave (see image below); that is not the case in the aforementioned case report. J-wave syndromes are proposed to give a unifying pathophysiology to Osborn waves of hypothermia and early repolarization, as well as Brugada syndrome.
Very large and wide J-waves, as in case 1, are almost exclusively due to hypothermia. The etiology is beyond the scope of this blog, but may be read here.
Hypothermia and pseudoinfarction patterns: MI or ischemia (either ST elevation or depression) may be mimicked either by 1) repolarization abnormalities (As in Case 2, with ST elevation) or by 2) confusing the J-wave with the ST segment, as in this case in JACC (full text) and this case in Archives of Internal Medicine (no full text). This latter case also has ST segment depression as a repolarization abnormality.
Short ST segment (with resulting short QT interval) of hypercalcemia mimicking Osborn waves
 |
| This image courtesy of Dr. K. Wang from his Atlas of Electrocardiography. The major difference between the Osborn wave and the example of hypercalcemia is that the Osborn wave is followed by an ST-T complex, while the wave directly following the QRS in hypercalcemia is the T-wave itself. |