A middle aged male presented at midnight after 14 hours of constant, severe substernal chest pain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. It was not relieved by anything. The pain was not positional, pleuritic, or reproducible. He had no previous medical history. The blood pressure was 110/60. Physical exam was normal and there was no murmur.
I delved into his reasons for arriving so late after onset, thinking that perhaps the pain had only recently increased, or that it had been intermittent until now, but he confirmed that it was 14 hours of constant pain and it was his significant other who insisted that he go to the ED.
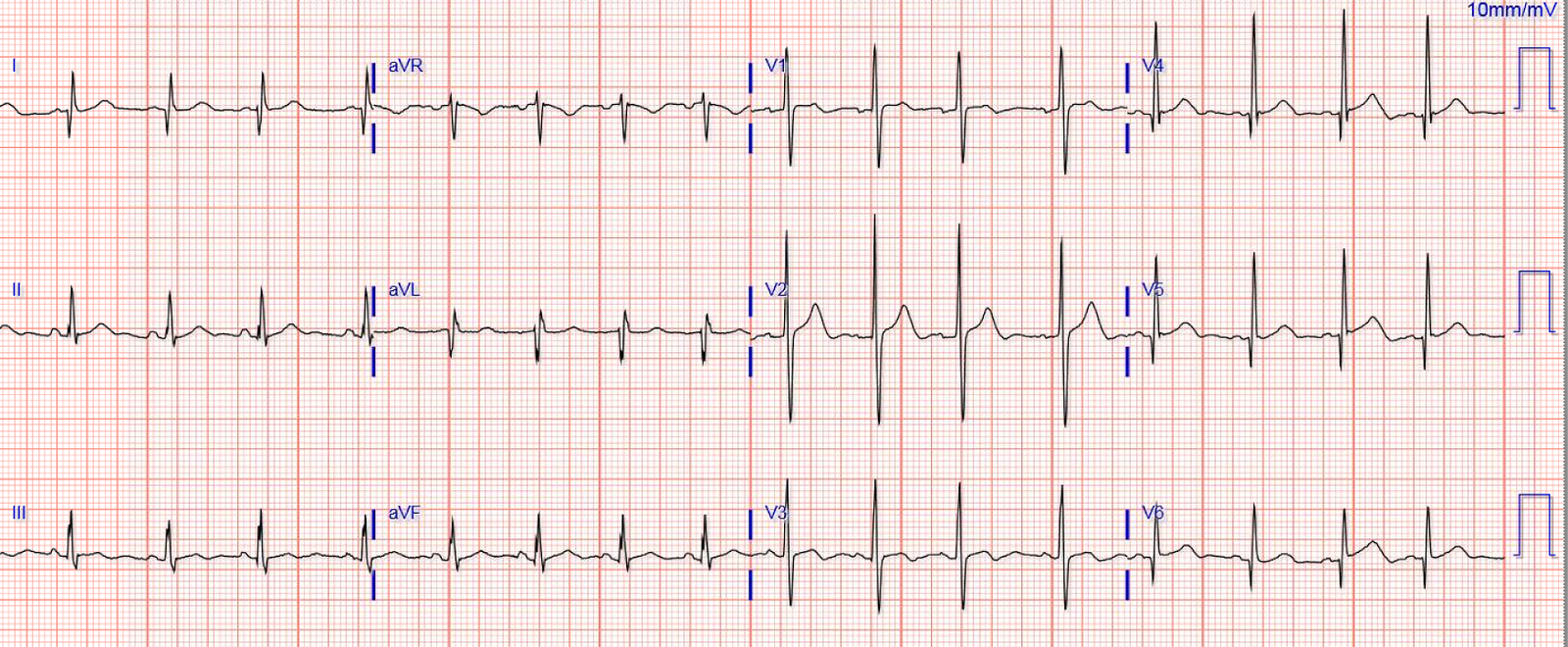
Here was his ED ECG:
 |
| I read this as normal
–One might say there is ST depression in II, III, and aVF, but this is merely an atrial repolarization wave. –You can see the PR segment sagging down, such that the PQ junction is also depressed. Thus, there is no elevation of the J-point relative to the PQ junction. –ST segment deviation is measured at the J-point, relative to the PQ junction –(“Inferior” ST depression would have told us that there is unseen ST elevation in aVL and be a strong clue to high lateral MI) |
I sent this to the Queen years later. She also could not see it:

He was given an aspirin and a troponin was drawn. If this is MI, then after 14 hours, the troponin should be elevated.
The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL), diagnostic of myocardial injury.
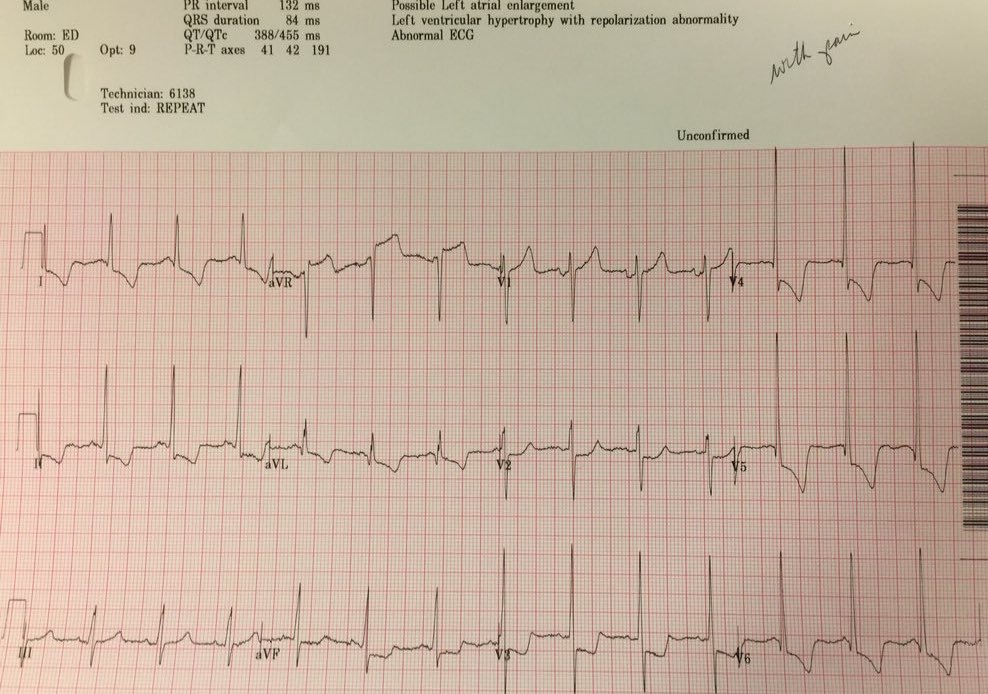
We recorded a posterior ECG:
 |
| V4-V6 are moved around to the back and are really V7-V9. The “criteria” for posterior STEMI are 0.5 mm STE in one lead. There is zero ST Elevation. There are tall R-waves in V2, which could be a sign of old or well developed posterior MI However, the ECG shows no evidence of acute MI whatsoever. |
We gave ticagrelor and heparin and sublingual nitro, with plans to start a nitro drip, but the BP dropped to 80/50 before the drip was started.
The pain was unrelieved.
What do you want to do?
The elevated troponin is diagnostic of myocardial injury. Is it acute or chronic?
There was a normal creatinine and no evidence of heart failure and no other reason for chronic injury, so it must be acute.
Acute myocardial injury:
Is it myocardial infarction, or perhaps myocarditis?
If it is MI, is it type 1 or type 2?
Is it STEMI or NonSTEMI?
Is it acute persistent occlusion?
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis.
The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We also looked at his aortic root by both parasternal and suprasternal views, and the aorta was normal.] The d dimer returned below the level of detection, ruling out PE and making dissection very unlikely.
So this was not a type 2 MI. And was not a PE or dissection.
A bedside echo showed good LV function but was inadequate to assess wall motion. We attempted Speckle Tracking Strain Echocardiography but could not get clear enough images without contrast.
We could not rule out acute epicardial coronary (large artery) occlusion.
What do you want to do now, considering you will need to awaken the hospital’s only catheterization team, which must be alert for the next long day in the cath lab?
I called the cardiologist on call and we agreed that we needed to activated the cath lab.
The patient was found to have an acute 100% occlusion of the circumflex proximal to 2 obtuse marginal branches. It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI).
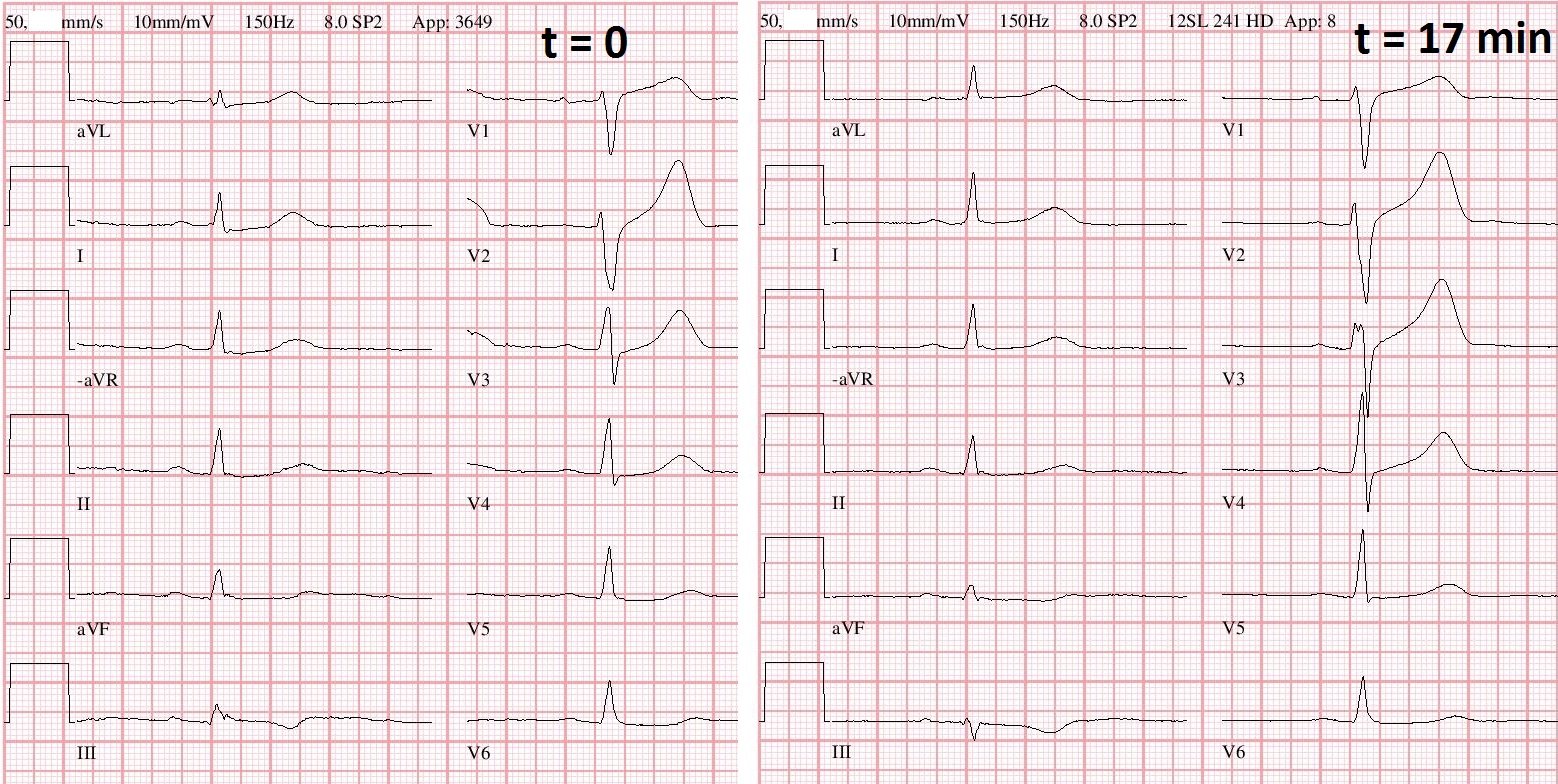
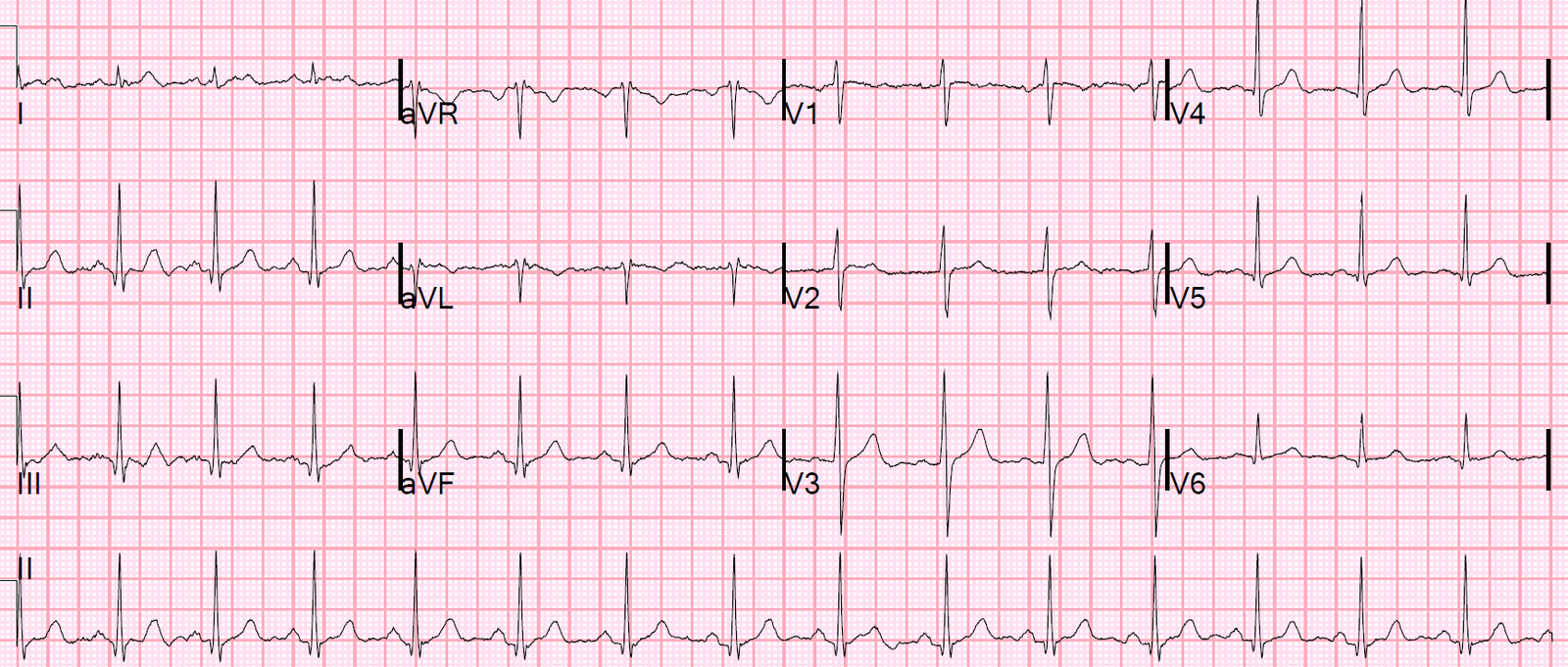
A post cath ECG is shown:
 |
| No significant change |
The third troponin, drawn before the artery was open, returned at 6.2 ng/mL.
The 4th, after the opening of the artery and release of troponin from the cardiac circulation, was 99.9 ng/mL
So this was a very large MI!!
The formal contrast echo the next morning was difficult technically but showed an inferior wall motion abnormality. It is unclear if this is “inferobasal” which is the new echo term for Posterior.
Learning Point
Acute coronary occlusion may occur with no ECG findings whatsoever. Some NonSTEMI require emergent cath lab activation to save viable myocardium at risk. A patient who has a high clinical suspicion of MI should go to the cath lab. This is not just my opinion, but the opinion of the American College of Cardiology and American Heart Association.
This is from the 2014 ACC/AHA guidelines. Earlier versions are more specific. “A subgroup
of patients with refractory ischemic symptoms or hemodynamic or rhythm instability are candidates for urgent
coronary angiography and revascularization.”
Here are the European Guidelines:
Timing of invasive strategy: Immediate invasive strategy (less than 2 h) in Very-high-risk NSTE-ACS patients (i.e. with at least one very-high-risk
criterion according to Table 13 (pasted below) have been generally excluded from
RCTs. Owing to a poor short- and long-term prognosis if left untreated,
an immediate (i.e. less than 2 h from hospital admission, analogous to
STEMI management) invasive strategy with intent to perform revascularization
is recommended, irrespective of ECG or biomarker findings.
This includes:
1. Patients with ACS and hemodynamic instability
2. Patients with ACS and acute pulmonary edema
3. Patients with ACS and electrical instability
4. Patients with ACS and refractory chest pain or refractory ischemic ECG findings, usually ST depression
A patient who presents with chest pain and an otherwise unexplained elevated troponin has acute MI. If the pain is refractory to medical management, no matter what the ECG shows, the patient should go emergently to the cath lab.