Unfortunately, the blogging software fails if I try to embed the EKGs in the text where they belong. Therefore, all EKGs will be at the beginning of the post.
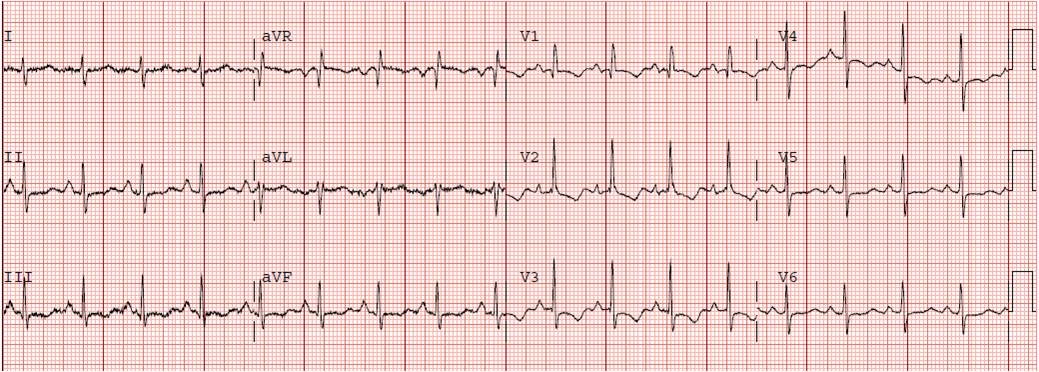
Initial ED ECG (#1):
This 55 yo male had no previous sigificant medical history. He began having chest pain at 6:30 AM and called 911. At 7:05 a prehospital EKG was recorded which is identical to EKG #1, and the cath lab was activated by the paramedics.
 |
| This EKG shows RBBB with a bit of ST elevation in aVL and V2, and upright T waves in V2 and V3 (these should be down in the presence of RBBB, and there should not be any ST elevation in RBBB). |
Anterior STEMI with new RBBB has very high mortality, even higher than with new LBBB.
The patient was very ill on arrival, with BP of 90. Wary of cardiogenic shock, we were preparing to intubate him quickly before sending him to the cath lab, but at that moment his pain resolved. On the way to the cath lab, the pain returned and the patient went into cardiogenic shock. His LAD was quickly opened (door to balloon time 50 minutes, and chest pain onset to balloon time of 100 minutes) but he remained very ill. A balloon pump was placed. An echo showed no serious valvular problems but had very poor ejection fraction with anterior and apical akinesis.
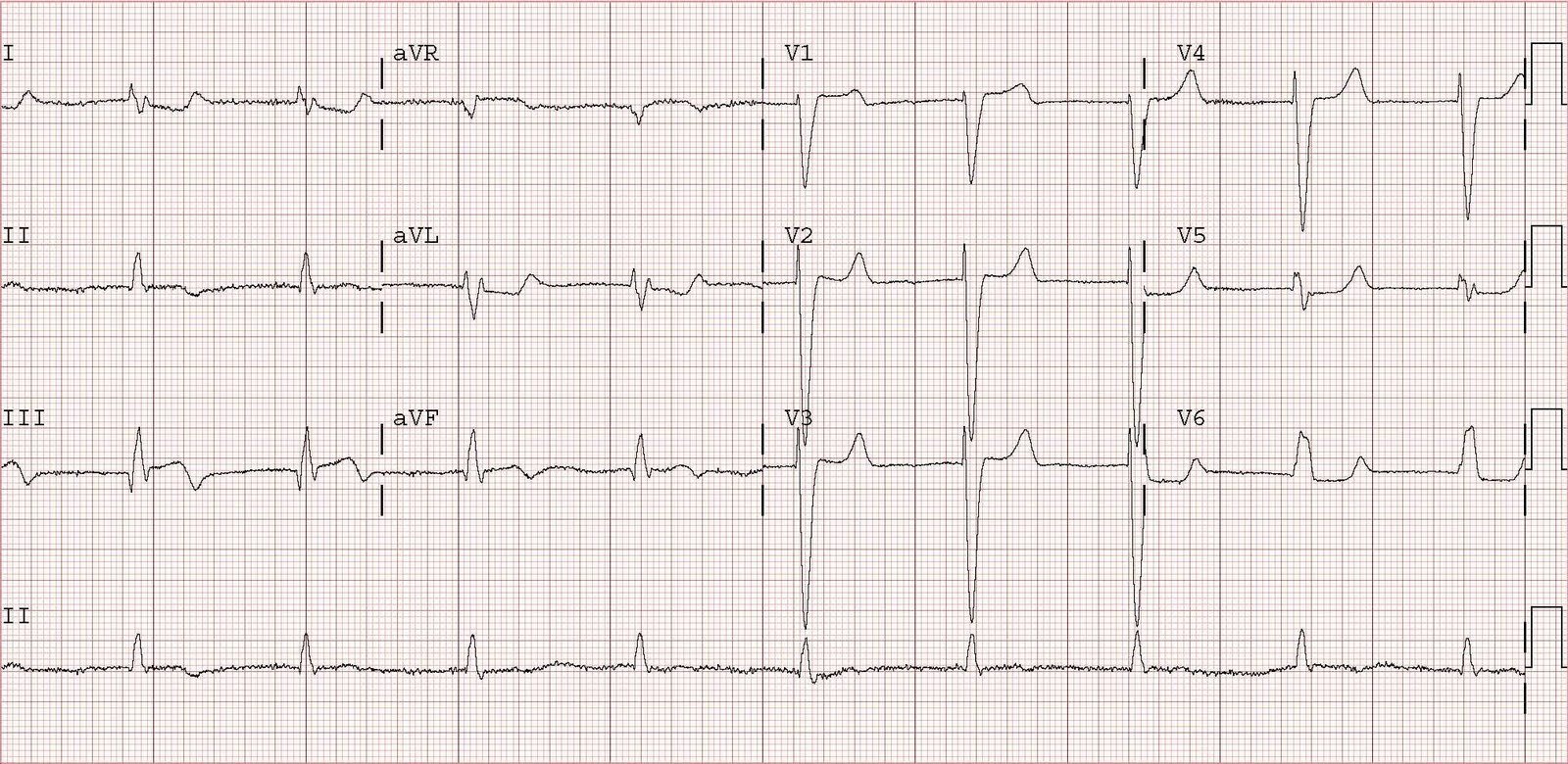
This ECG was recorded after the procedure:
 |
| There is at least 2 mm of persistent ST elevation. The RBBB has resolved. Persistent ST elevation after opening of the infarct related artery is a sign of poor downstream perfusion with microvascular obstruction due to platelet fibrin coagulates as measured by TIMI myocardial perfusion grade, or “blush”. It is associated with a poor outcome and development of LV aneurysm. On the other hand, resolution of BBB that was caused by ischemia is a good sign. |
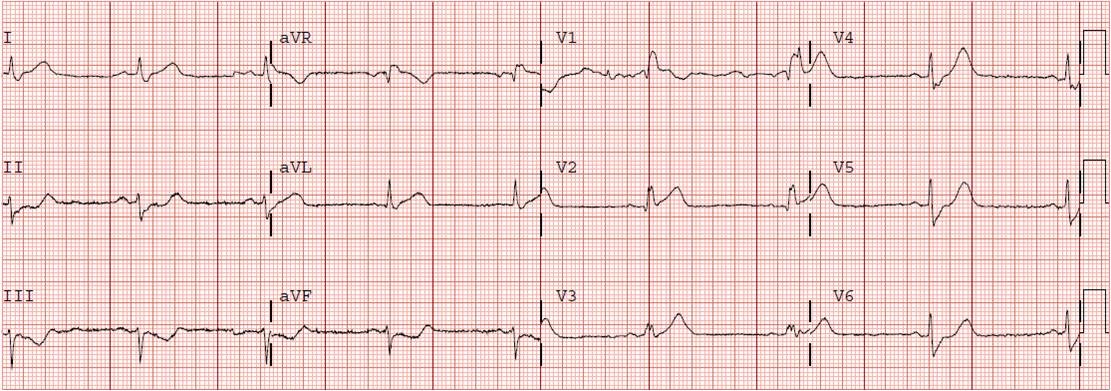
This ECG was recorded on day 2:
 |
| There is persistent STE and QS-waves in V2 and V3 |
Max troponin I was 99 ng/ml, which is high for such a short onset to balloon time, but consistent with microvascular obstruction. Frequently in such cases, ST elevation will persist indefinitely and the patient will develop a ventricular aneurysm, often complicated by a mural thrombus. In the pre-reperfusion era this was very common, and could even be complicated by myocardial rupture (which is really a small leak) and pericardial tamponade.
.
EKG #4 was recorded one week later:
 |
| There is now recovery of some anterior electrical forces, with an R-wave in V3 where there was a Q-wave and resolution of almost all ST elevation. |
At this time, the patient was clinically much better, his echo showed recovery of the anterior wall and apex, his ejection fraction was up to 45%.