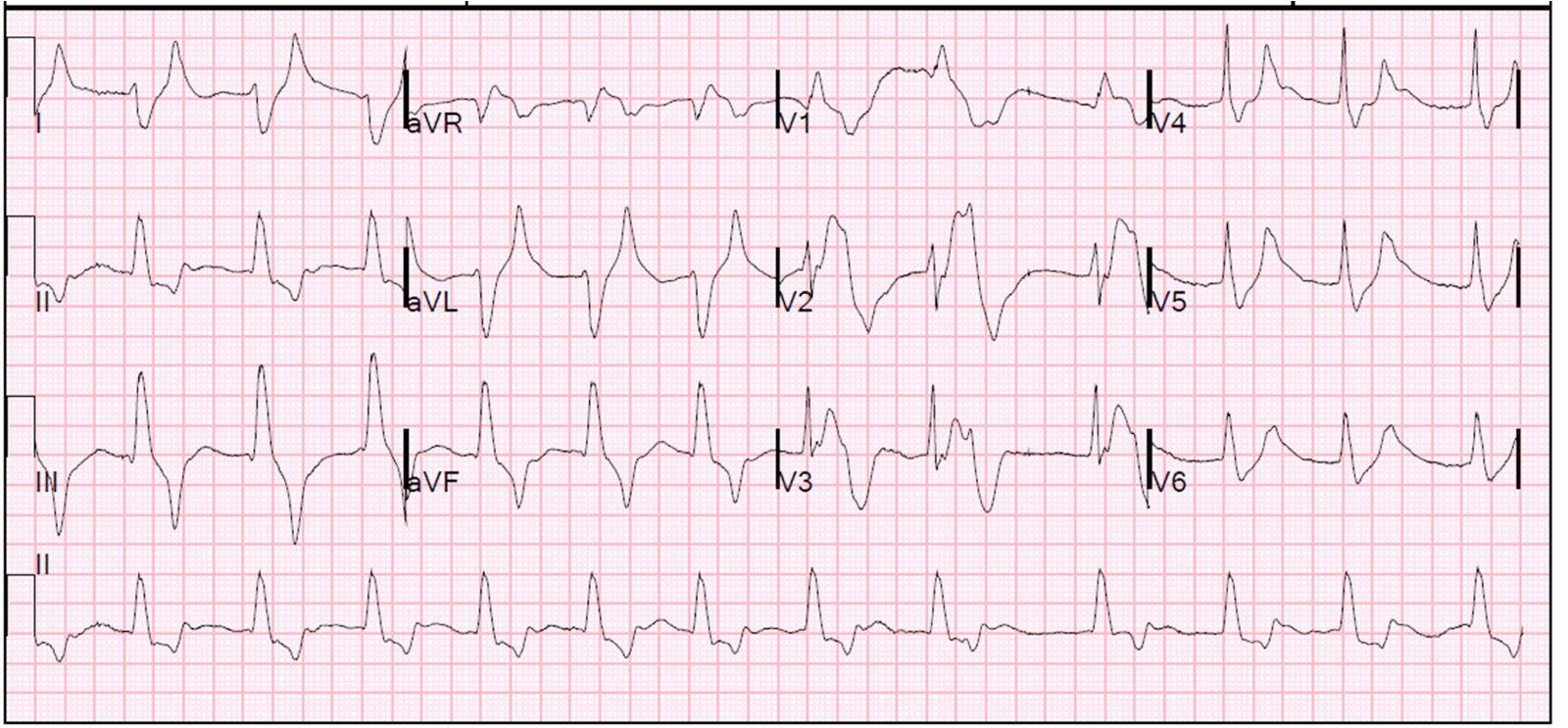
This 65 yo male presented with 24 hours of intermittent and low grade chest pressure. Here is the presenting ECG:
There is ST depression with upright T-wave in leads V2-V6, maximal in V3. There is no ST elevation anywhere on the ECG. There are those who deny the existence of posterior STEMI; they argue that coronary anatomy makes it “extremely unlikely.” But fact has a way of overturning theory.
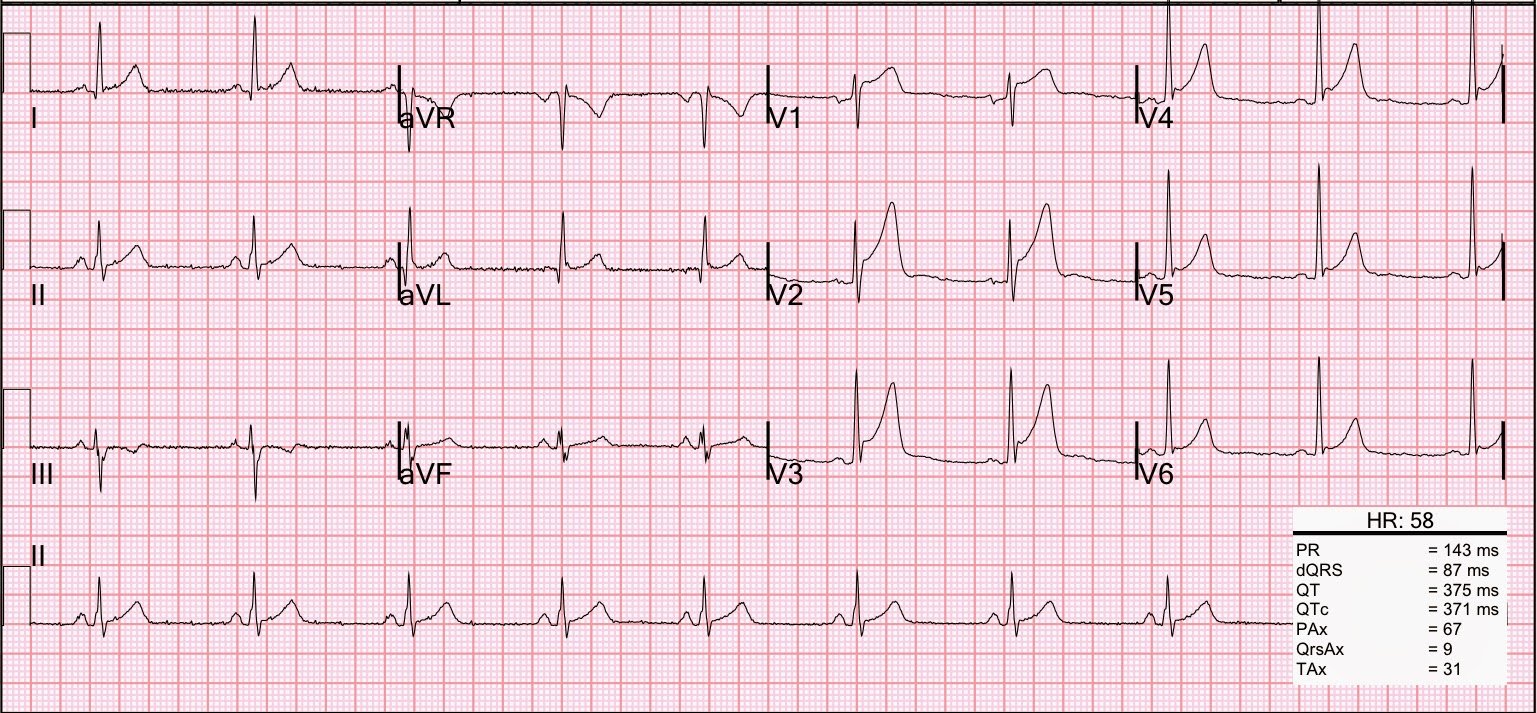
After therapy with IV nitroglycerine and an aspirin, the ST depression and chest pain resolved. Because of issues with some contraindications to antiplatelet and anticoagulation therapy, and because the ECG and symptoms had resolved, he was not taken immediately for cath. He did have an echo confirming a new posterolateral wall motion abnormality.
Next day cath showed a 100% Ramus intermedius occlusion; it was opened and stented. Max TnI was 14 ng/ml. Echo showed corresponding new WMA and EF was 54%.
There are many studies that indirectly reveal that the percent of STEMIs that are isolated posterior is between 3 and 11% (about 8%). More recently, a substudy of the recent TRITON-TIMI 38 trial comparing Prasugrel to Clopidogrel for ACS enrolled 13,608 patients; 1198 had isolated ST depression in V1-V6. Of these, 314 (26%) had occlusion (TIMI 0 or 1 flow) of the infarct-related artery (i.e., STEMI).
There were 3534 other STEMIs in this study, not including the 314 with ST depression only (posterior STEMI). Add these 314 to the 3534 and you have 314/3848 (8.1%) of STEMI have pure isolated posterior STEMI. This conforms with the previous smaller studies. Moreover, the cath was done a median of 29.4 hours after presentation, so this does not account for those arteries that spontaneously reperfused (about 25% of STEMI will reperfuse with antiplatelet and antithrombotic therapy alone within one day — old data). Thus, there were probably even more occluded arteries.
Only 14/314 (4.5%) were interpreted by the investigator as STEMI. None of the patients with an occluded artery had an ECG to PCI time <6 hours. This is not a "rare" event.