56 y/o male who presented with 12/10 severe chest pain starting at 3AM, radiating to his upper back. He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different.
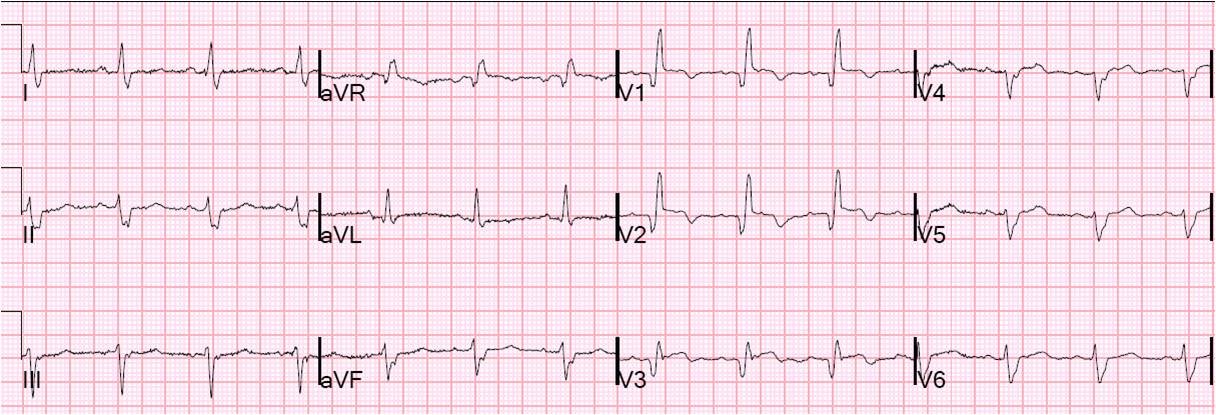
His baseline ECG from 10 months before is normal. Here is his initial ECG at 0831:
 |
| There is sinus rhythm with RBBB. There are upright T-waves in V2 and V3, with a slight amount of ST elevation in V3. In RBBB, T-waves are usually inverted in V2 and V3, with some ST depression. (See ECG below) Any ST elevation is abnormal. There is also some STE in lead II, and insignificant STE in III, without any reciprocal ST depression in aVL. |
Here is what V1-V3 should look like in RBBB:
 |
| Notice inverted T-waves, discordant to the majority of the QRS (the R’ wave is the majority) and a small amount of discordant ST depression |
He continued to have severe pain, so more ECGs were recorded, at 0927 and 0942:
 |
| There is increasing ST elevation in inferior leads without ST depression in aVL, and dynamic T-waves in V2 – V4. |
 |
| Not much change from 15 minute prior, but abnormalities are persistent. |
Here are V1-V3 from the last 3 ECGs:

It is now clear that there is cardiac ischemia. Inferior? Anterior? Both? Wraparound?
The patient was very hypertensive and had back pain, so they did a CT of his chest to rule out dissection. It was negative.
Because of the dynamic T-waves and crushing chest pain, he went directly to the cath lab where they found an open wraparound LAD with a large dangerous thrombus.
The peak troponin I was only 10 ng/mL and the patient did well.
Serial ECGs and close attention saved his anterior wall.
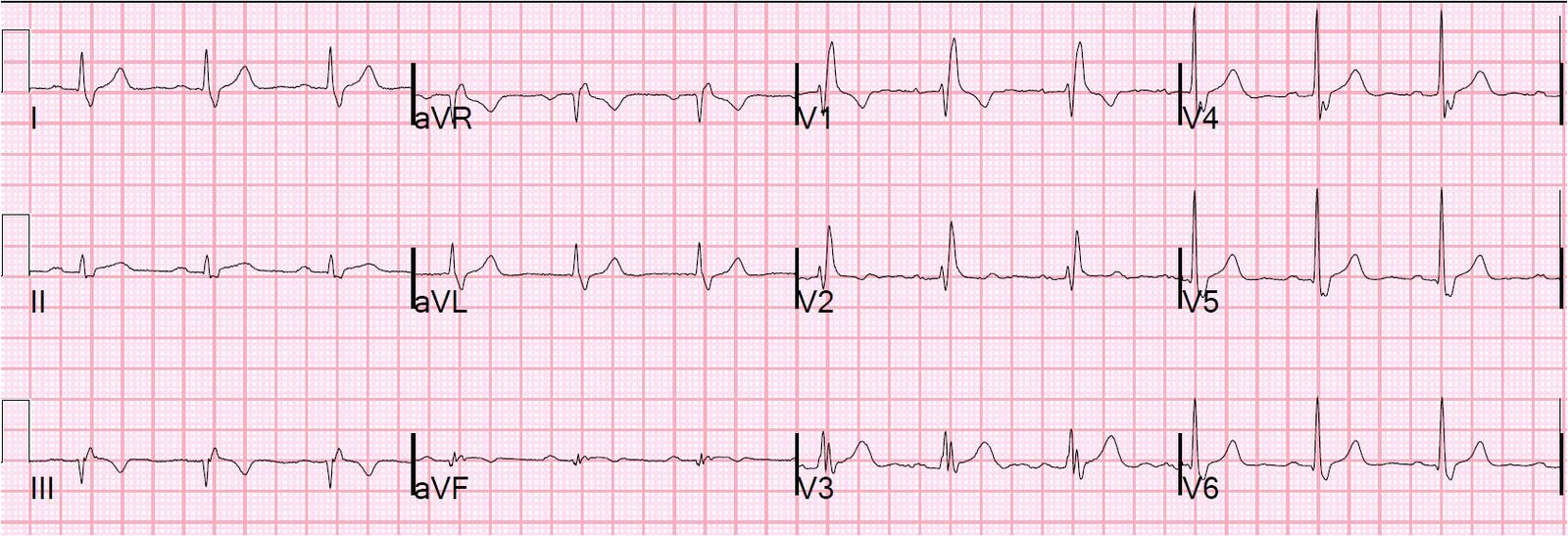
Here is the post PCI ECG:
 |
| T-waves are still upright. |