An elderly woman was brought to the ED for hypoxia. She had a history of chronic respiratory failure with a tracheostomy and had had multiple episodes over the past few days of increased respiratory effort and hypoxia (down to an SpO2 in the 70s on supplemental O2 via nasal). Associated with this has been increased secretions requiring aggressive suctioning.
On exam in the ED, the patient did not appear nearly so ill and was not hypoxic.
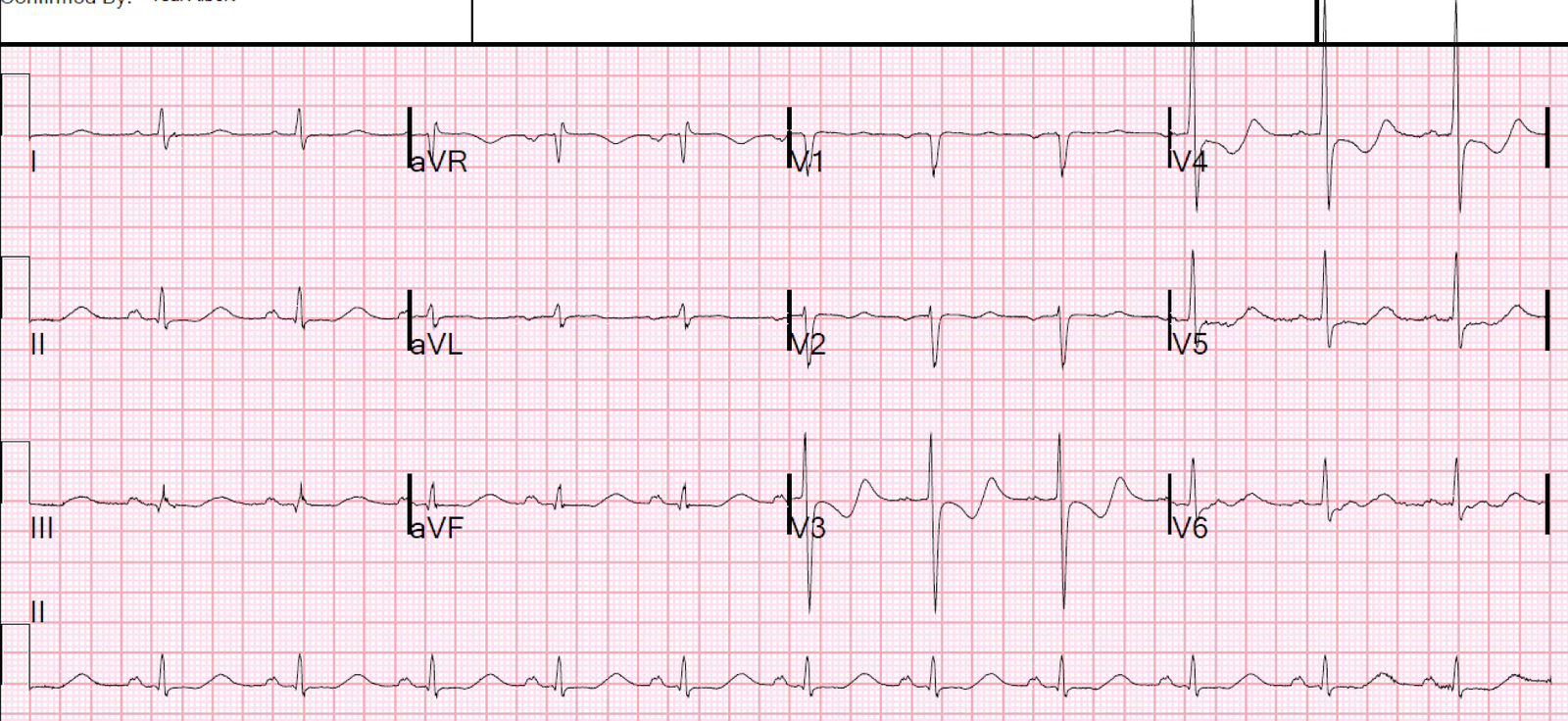
A routine ECG was obtained:
 |
| There is inferior and lateral ST elevation with hyperacute T-waves, and reciprocal ST depression and T-wave inversion in aVL. This is all but diagnostic of STEMI and should be considered to be so until proven otherwise. |
The cath lab was activated.
She was given a full dose of aspirin and a heparin bolus of 4000 units. A repeat ECG demonstrated no dynamic changes. Bedside cardiac ultrasound had grossly normal systolic function with no apparent wall motion abnormality.
Because the patient had no symptoms specific to STEMI and an ECG that was not evolving, and while waiting for the cath lab to be ready, the very astute providers sought out a previous ECG and were able to get one faxed from another hospital.
It looked exactly the same!
So they waited for the first troponin and it was below the level of detection.
They decided against an angiogram.
The patient ruled out for MI by serial troponins.
This turned out to be the patient’s baseline ECG!
Learning Point
Rarely, a patient’s baseline ECG looks just like a STEMI. It never hurts to find a previous one unless it delays care.