A 60-something was outside walking with a friend when he suddenly stated that he “felt weak,” without chest pain or SOB or headache, and dropped to the ground, pulseless. She did CPR and called 911. When medics arrived he was pulseless and the monitor showed a slow wide regular pulseless rhythm.
After several minutes of excellent resuscitation, they achieved ROSC.
In the ED, he was intubated, TTE showed very poor cardiac function, and a TEE was placed, as well as arterial line and central cooling catheter.
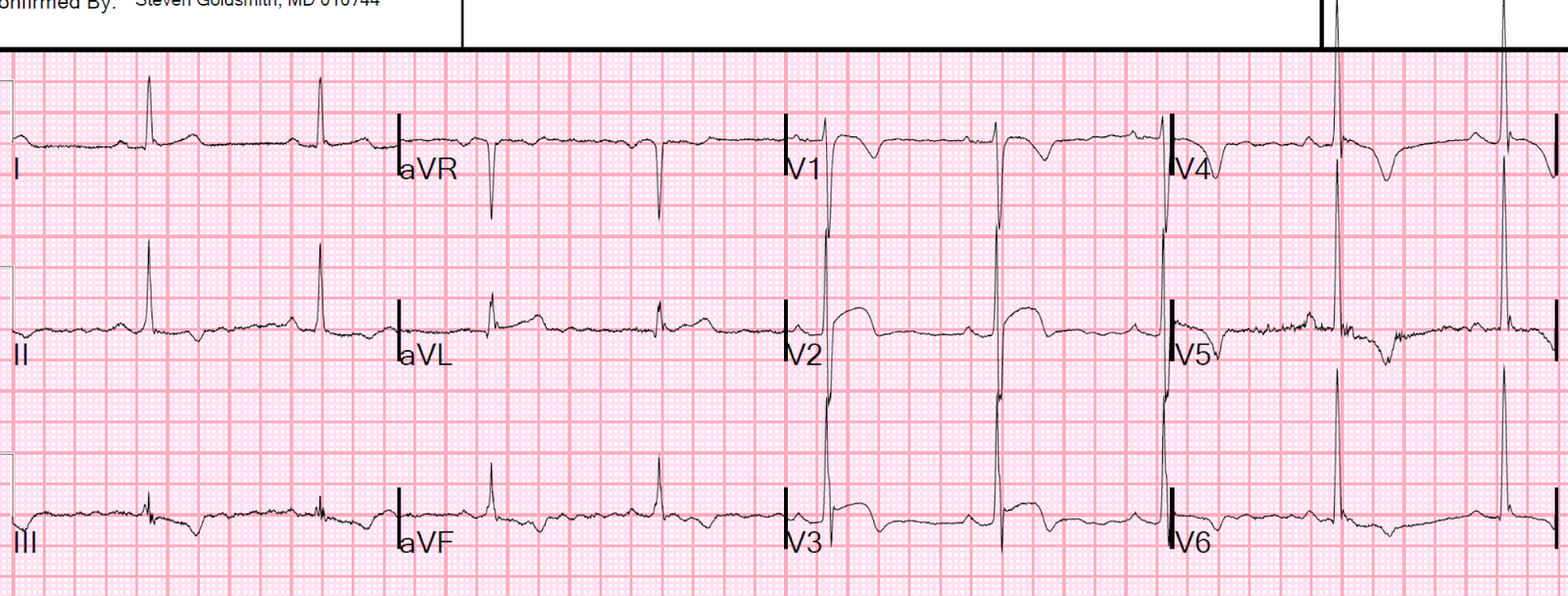
Here was the first ED ECG:
 |
| There is sinus tach (see the P-waves in V1? The small up-down waves?)
The P-waves in lead II are superimposed on the T-waves. There is a nonspecific intraventricular conduction delay. There is no clear evidence of OMI. There is some ischemic ST depression in V4-V6, but it is not profound. |
Here are causes of sudden cardiac arrest, and relevance to this case (H’s and T’s):
- Hypoxia — does not fit
- Hypovolemia — Causes would be GI bleed, Rupture AAA, other ruptured vessel such as mesenteric aneurysms. None of these fit for such a sudden arrest
- Hypothermia — does not fit
- Hypo/hyperkalemia — K was normal
- Hydrogen ions — Lactate was 8 in spite of being measure after arrest. Anyway, life-threatening acidosis does not happen so rapidly
- Hypoglycemia — this is a reason to have coma, but not sudden cardiac arrest
- Thrombosis – coronary or pulmonary — either of these are likely culprits
- Tamponade – cardiac — ruled out immediately by echo
- Toxins — is there any toxin that causes arrest so fast? Cyanide?
- Tension pneumothorax — doesn’t fit, and patient was ventilating well, had breath sounds, and sliding signs.
- Trauma — History doesn’t fit.
Coronary or Pulmonary Thrombosis
–Pulmonary embolism: did not fit, as the TEE showed a lot of B-lines and the RV was normal
–He had been well until the moment of weakness.
The only explanation in my mind was a sudden massive coronary occlusion, such as left main. When occluded, the heart can just stop functioning. The heart might just stop beating, without dysrhythmia (without VT or VF).
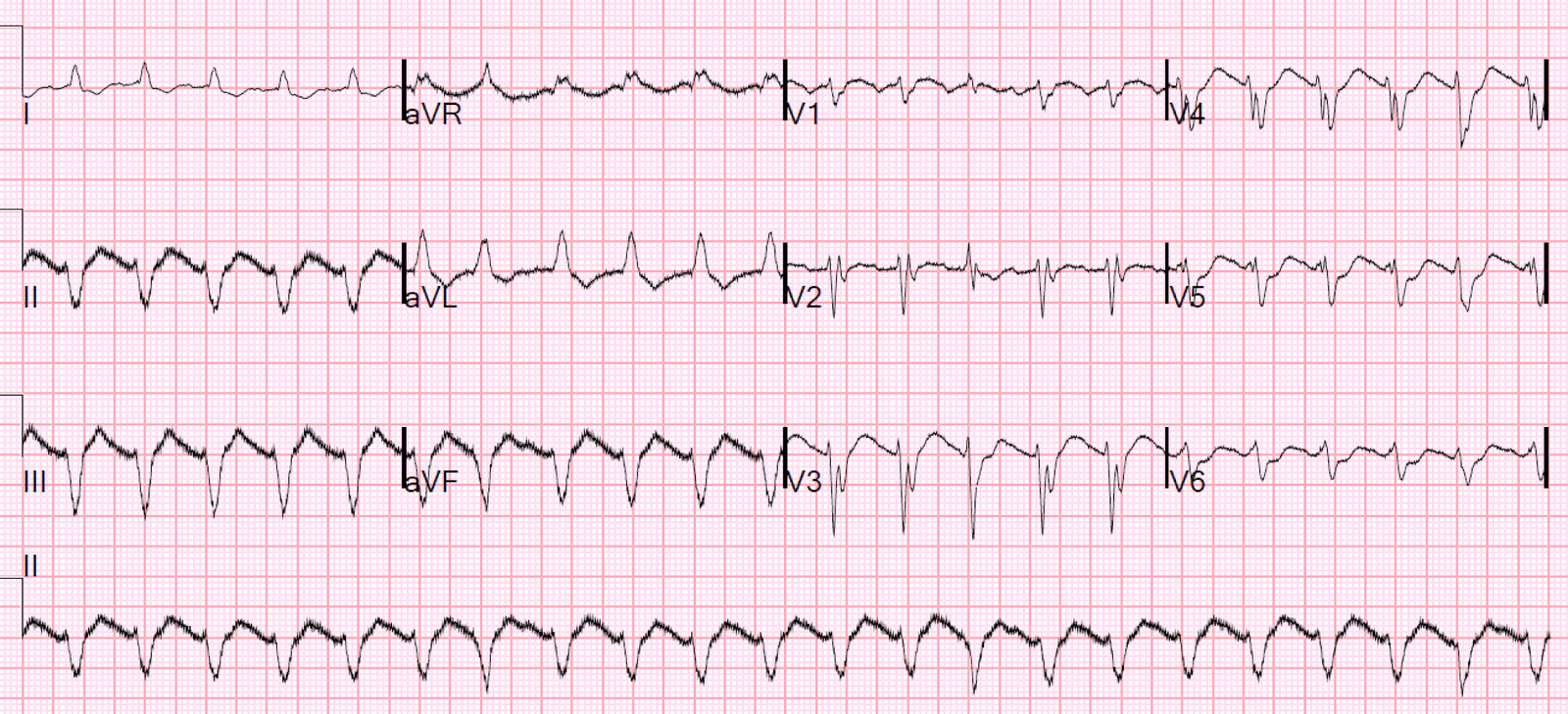
How do I know he didn’t start with a VF arrest? Because his initial rhythm was organized. VF does not re-organize itself except in very rare circumstances:
This is an amazing case for many reasons:
Ventricular Fibrillation During Echocardiogram, Then Spontaneous Conversion Without Defibrillation
Case continued
I had just requested a cardiology evaluation for emergent angiogram in the absence of STEMI when he had another arrest.
We resuscitated him again, and he was then more hypotensive and in atrial fib with RVR, so we cardioverted to a regular rhythm, which helped with perfusion.
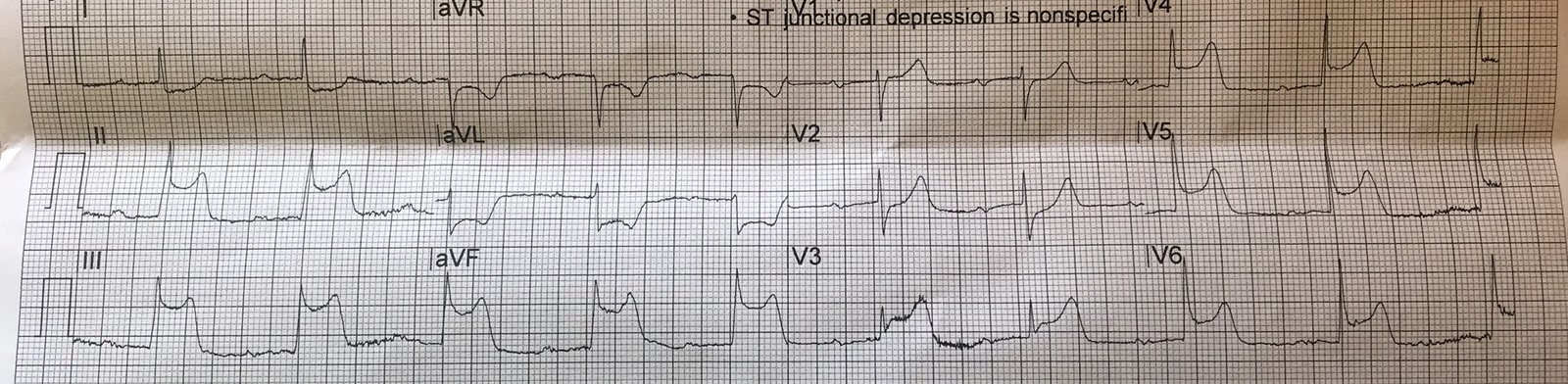
Here is the 12-lead ECG after re-arrest:
 |
| What is the rhythm? Is it ventricular tachycardia (VT)?
Is there any evidence of OMI? Rhythm One might think this is VT, but if you look at beats 15 and 16 across the bottom, they are PVCs, and the 2nd PVC is followed by a P-wave and then a conducted beat, proving that the rhythm is sinus rhythm. If you assess the PR interval, then go to other complexes, you can see that the P-wave in the first 14 complexes, and in 18-23, is superimposed upon the T-wave. QRS? Appears to be RBBB and LAFB (a very bad combination, often associated with left main thrombosis) OMI? There is no clear ischemic ST Elevation. Inferior leads have what may seem to be ST Elevation, which should not occur in RBBB. And aVL appears to have some ST depression However, if you look closely, the J-point really is isoelectric |
The fact is that the ECG commonly fails to show evidence of OMI. In this recent large study of consecutive chest pain patients, ST elevation was only 21% sensitive for OMI, and 6% sensitive for any acute MI. We have submitted a manuscript showing very poor sensitivity of the ECG for OMI in cardiac arrest patients with a shockable rhythm who were resuscitated.
Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
There has long been controversy about whether to take patients with a shockable rhythm without ST Elevation to the cath lab, and a recent randomized trial showed no benefit: Coronary Angiography after Cardiac Arrestwithout ST-Segment Elevation (COACT)
This study had a fatal flaw: they did not keep track of all the Non-STEMI patients who were NOT enrolled, but instead were sent for immediate angiogram. It was done in Europe, where the guidelines suggest taking all shockable arrests emergently to the cath lab. So it is highly likely that physicians were very reluctant to enroll patients; they did not want them to be randomized to no angiogram. This strong suspicion is supported by their data: only 22 of 437 (5.0%) patients in this study had OMI.
What percent of shockable arrests without STE have an OMI?
This large registry in Circulation 2010 reported that at least 1 significant
coronary artery lesion was found in 128 (96%) of 134 patients with ST-segment elevation on the
ECG performed after the return of spontaneous circulation, and in 176 (58%) of 301 patients without ST-segment elevation.
5% vs. 58%!! So there is definitely enrollment bias.
The etiology of arrest in non-shockable rhythms is much less likely to be OMI (I don’t know the exact number here).
Even though most OMI causes VT/VF, when the ischemia is overwhelming, such as in Left Main occlusion or near-occlusion, the heart may just stop beating.
Seeing no other etiology than OMI, and knowing that the only chance for survival was to find and open a coronary artery, I activated the cath lab.
He was taken to angiogram in a very unstable condition on an epinephrine drip. The angiogram showed:
LM: 90%
LAD: 100%, probably chronic
RCA: moderate to severe proximal RCA, and acute distal rPLA1 100% (probable acute) occlusion. Prior to occluding, it was supplying almost the entire territory of the left main through collaterals.
The LM and rPLA1 were stented.
The patient stabilized.
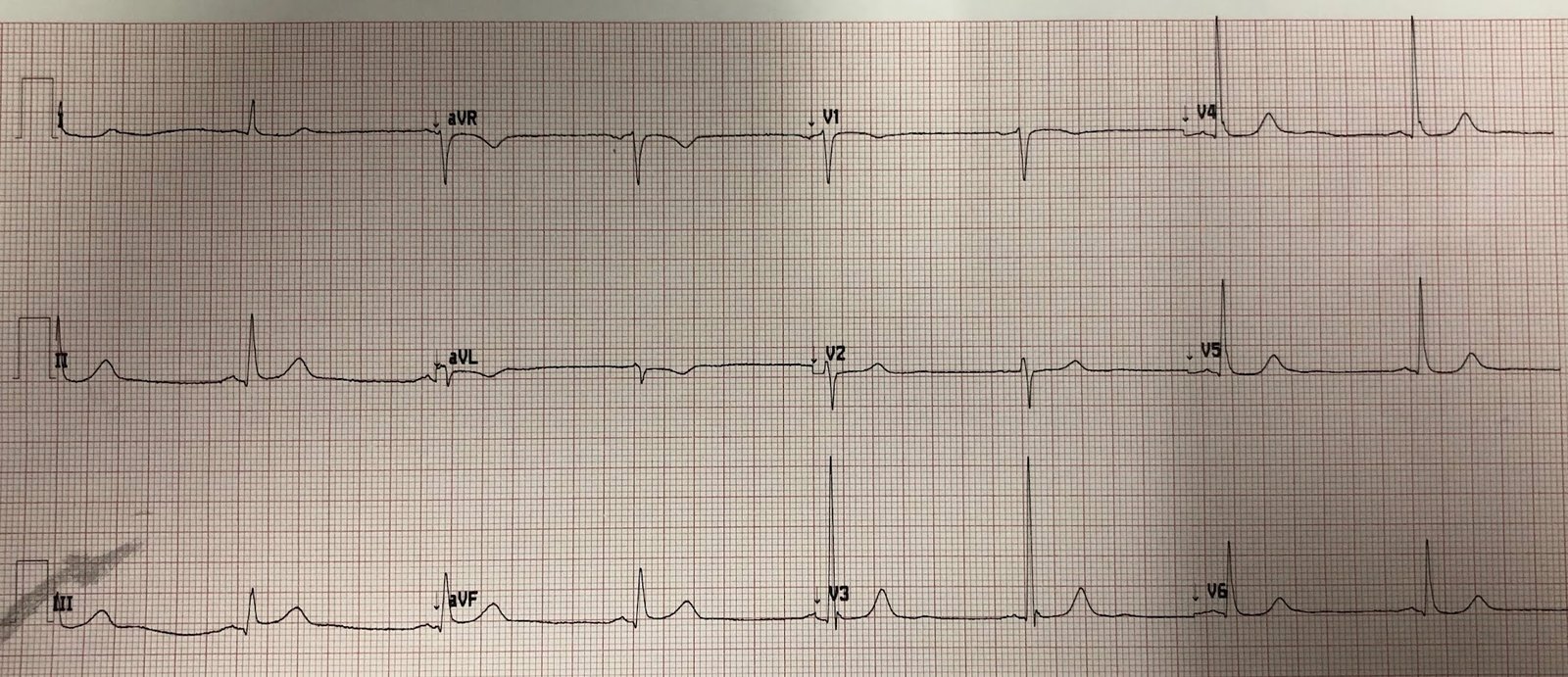
After PCI

Outcome
The patient had an unstable course but did wake up and stabilized but with severe ischemic cardiomyopathy, EF 15%.
Learning Points:
The pretest probability of OMI in cardiac arrest is very high. In patients with chest pain, only 1-5% have OMI, so the negative predictive value (NPV) of the ECG is pretty high, even though the sensitivity of the ECG for OMI is low. In shockable cardiac arrest, and in non-shockable cardiac arrest without any other etiology, the pretest probability of OMI is very high, so the NPV of the ECG is very poor.
More literature
In this 1997 NEJM study, 48% of shockable ROSC cardiac arrests were due to coronary occlusion; 1/4 of these had no ST elevation. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest
We have submitted a study of the ECG in shockable resuscitated cardiac arrest: My sensitivity and specificity for occlusion on the angiogram was 75% and 85%. The cardiologist who read the same ECGs had sensitivity and specificity of 62% and 77%. So even I cannot see 25% of OMI on these ECGs.
Interestingly, the 2nd ECG, after stabilization, had an overall sensitivity for OMI of only 26%!!