I was reading from our list of unconfirmed ED ultrasounds and saw a cardiac ultrasound with good LV function, but with B-lines of pulmonary edema, pleural effusions, and a very dilated inferior vena cava.
So I went to look at the chart.
It was a chronically ill patient with sepsis, a heart rate of 120, presumed sinus tachycardia, and did not have chronic renal insufficiency.
But there was no ECG recorded.
It did not make sense to me that someone who was septic would have ultrasound evidence of fluid overload unless they had renal failure, which this patient did not.
Then it turned out that an ECG was recorded upstairs, but only after admission:
 |
| What is it? |
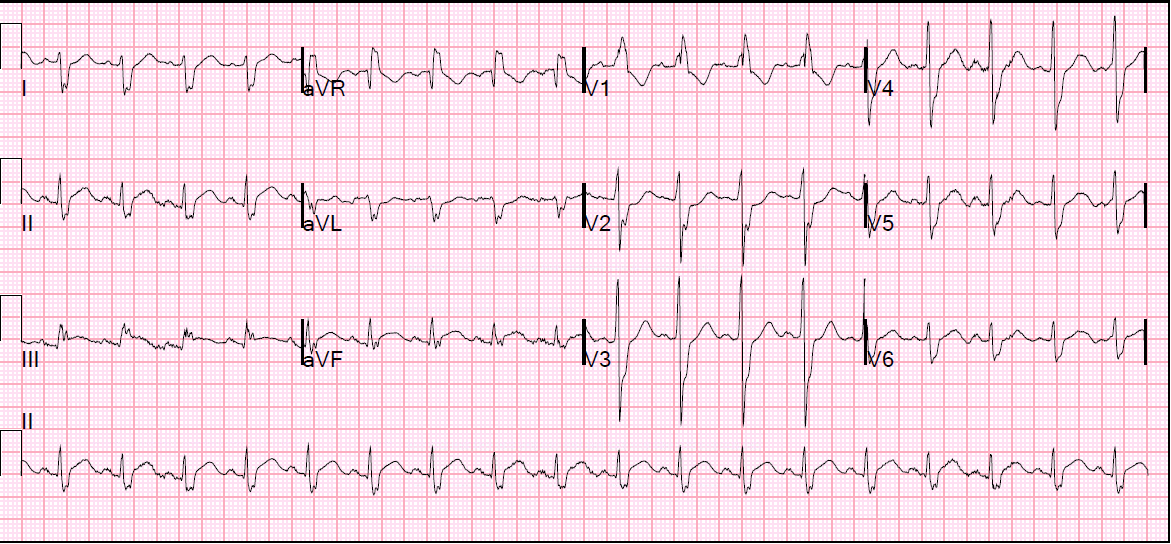
This is atrial flutter at a rate of 120.
This was not only recorded late, but misread as sinus tachycardia.
The giveaway is the upright P-wave in lead V1.
Sinus P-waves always have a negative component. The right atrial component comes first and is upright, the left atrial component comes next and is negative, such that the P-wave in V1 should be biphasic. Upright P-waves in V1, as in this ECG, are classic for atrial flutter.
See these posts for slow atrial flutter:
—Tachycardia with Pericardial Effusion
—A Very Wide Complex Tachycardia. What is the Rhythm? Use Lewis Leads!!
—Very Fast Very Wide Complex Tachycardia
—Several Wide Complex Rhythms in One Patient. Test yourself: Will You See What I Did Not See?
Discussion
The clinicians probably did not consider that tachycardia at a rate of 120 in a septic patient might be something other than sinus tachycardia.
Just recording a 12-lead on an ill patient may reveal the unexpected. Atrial flutter commonly comes in atrial rates as slow at 240 (and ventricular rates as slow as 120), and even slower in the presence of sodium channel blocking drugs.
Also, pulmonary edema should raise high suspicion of a cardiogenic cause, and this is due to either pump function (systolic vs. diastolic), valvular dysfunction, or dysrhythmia. The patient had good pump function, and sepsis usually leads to volume depletion, or relative volume depletion. Thus, the pulmonary edema had to be either noncardiogenic (or pneumonia), or due to either dysrhythmia or valvular disease.
Most dysrhythmias are easily diagnosed by ECG.
Learning Points:
1. Always record a 12-lead on a sick patient
2. Flutter can be at rates much lower than you expect.
3. Flutter often mimics sinus tachycardia
4. Fluid overload must be explained, and a cardiac cause is very likely. This is especially true in clinical situations in which volume depletion is expected.