This 86 year old woman had syncope. There is no chest pain or SOB. She is uncertain of her past medical history.
 |
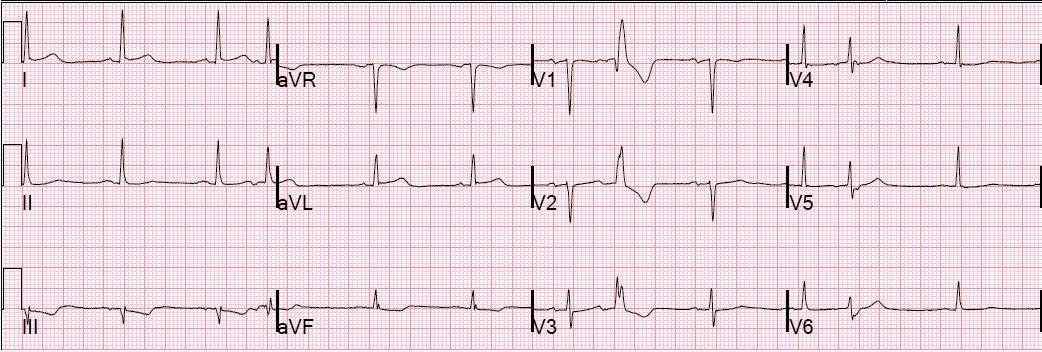
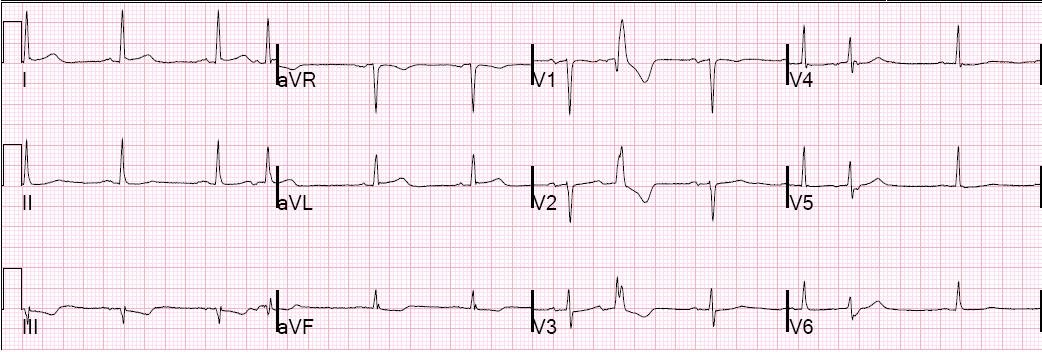
| There is atrial fibrillation and profound ST depression. What else do you see? What else do you want to know? |
Answer below:
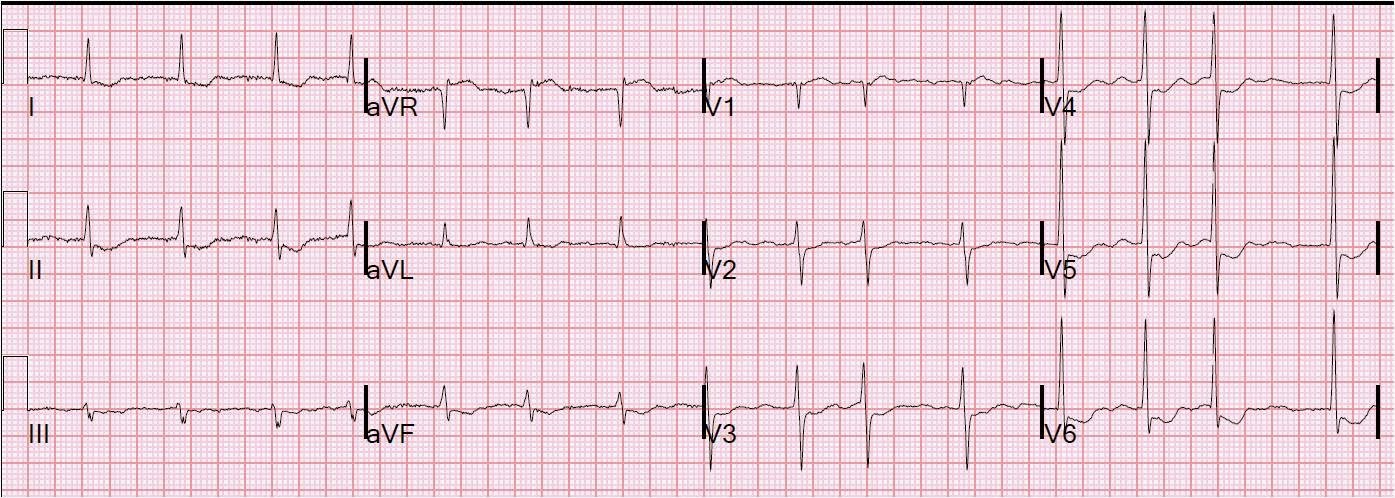
Here is the same ECG with some arrows:
 |
|
|
Any patient in atrial fibrillation might be on Digoxin. Etiologies of ST depression with a normal QRS (“primary” ST depression, in contrast to “secondary” ST depression that is due to abnormal QRS such as in LVH, LBBB, RBBB, WPW, hyperkalemia, Brugada, RVH, or paced rhythm) include hypokalemia, digoxin, and ischemia, as well as baseline ST depression of unknown etiology.
Digoxin results in ST depression with a short QT and often with prominent U-waves such as in this case. Hypokalemia results in a long QT with prominent U-waves.
Ischemia results in ST depression with a relatively long QT, and is likely to be accompanied by ischemic symptoms. Syncope is not an ischemic symptom; it is a relatively rare sole manifestation of ischemia.
It is important to keep in mind that ST depression due to digoxin happens at therapeutic concentrations, and is not a sign of Dig toxicity.