This was sent by a very good medical student, who had a very good question. He wishes to remain anonymous.
A 56 y/o male presented with Chest Pain radiating to the left jaw, starting at 8pm
the previous night (15 hours prior), which was 10/10 at that time. He decided to wait it out at home, then presented
at around 11 AM, pain now reported at 2/10.
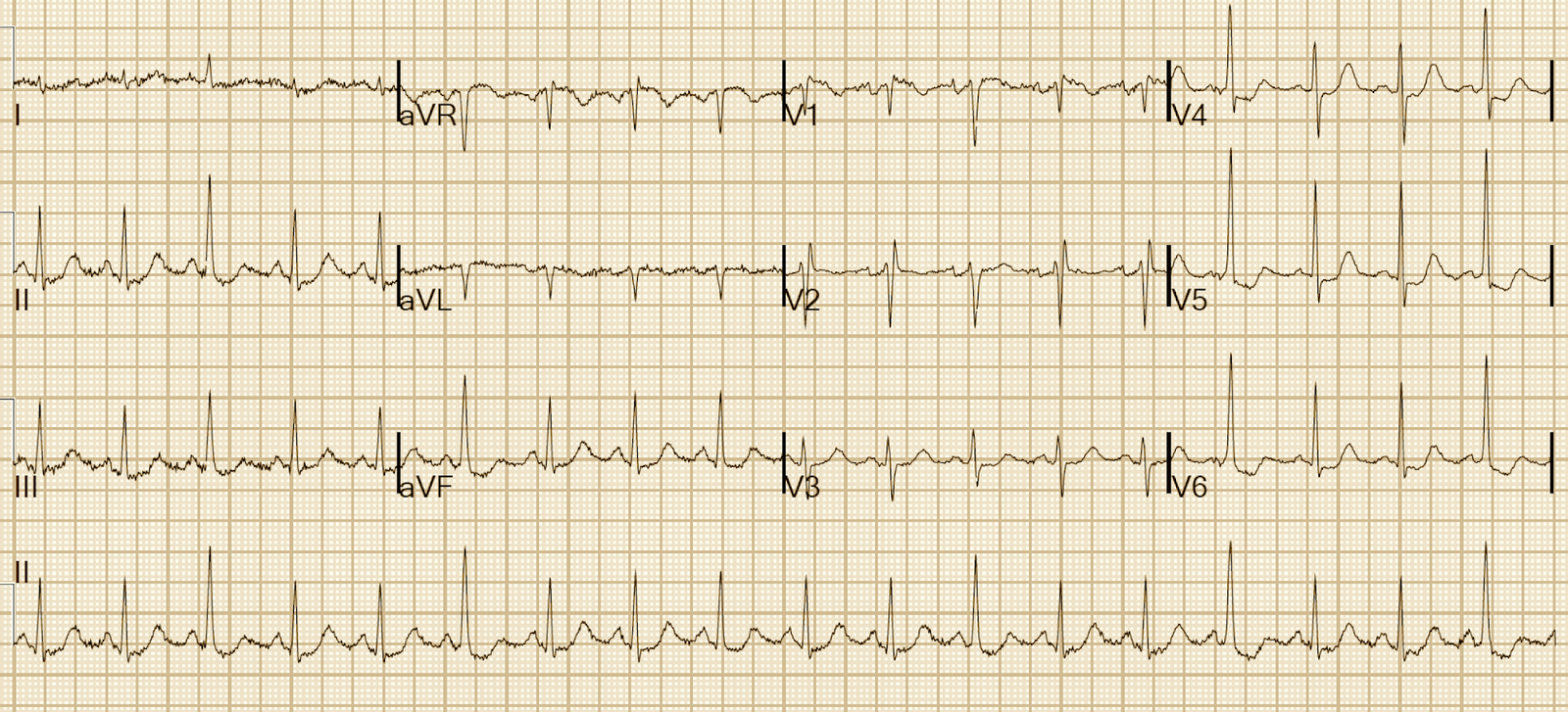
Here is the initial ECG (see the patient’s previous ECG below for comparison):
 |
| There is sinus rhythm and new inferior QS-waves with less than 1 mm of inferior ST elevation, and reciprocal ST depression in aVL, and T-wave inversion. |
Such T-wave inversion is common not only in reperfusion, but in persistent and prolonged occlusion after formation of Q-waves, especially QS-waves.
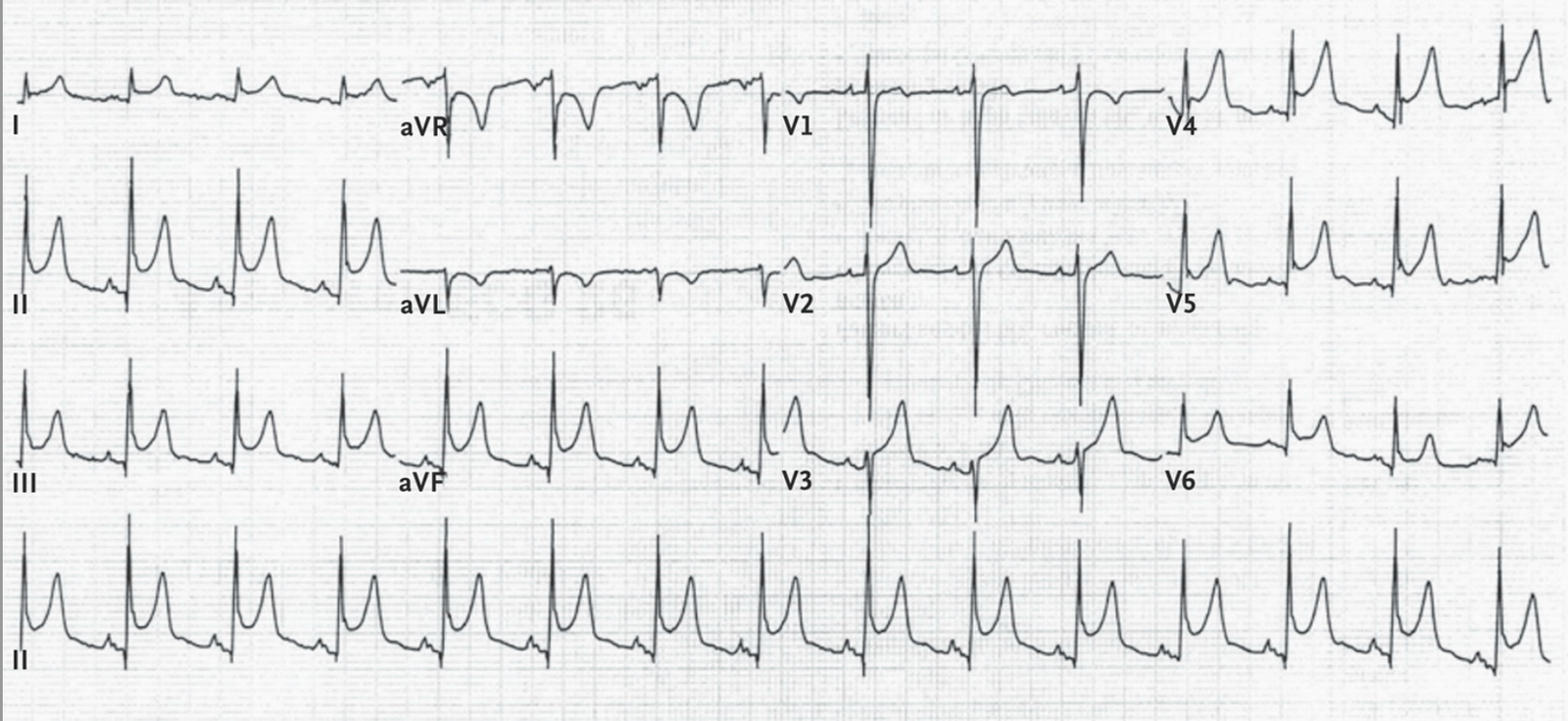
Here is the patient’s previous ECG:
 |
| This old ECG confirms that the first ECG shows a new MI |
So this patient has a subacute STEMI.
The initial troponin T returned at 0.47 ng/mL (quite high for Troponin T) and rose from there to 0.81, then 1.96 (typical of a large STEMI). Whether the troponin continues to rise or not says nothing about ongoing ischemia: it takes time for complete troponin rise and fall even after infarction is completed. Only the ECG and pain can tell you prospectively whether ischemia is ongoing.
The patient was admitted with “NonSTEMI” and did not undergo emergent angiogram and PCI. He went the next day.
This is a nearly completed STEMI (a very advanced subacute STEMI). To call it a NonSTEMI is misleading.
Is it too late for emergency cath lab activation? Should he go now, or with less urgency (tomorrow)?
My answer is this:
If there is:
1) persistent ST elevation (as there is here) or
2) persistent pain (as there is here)
Then the patient should go emergently.
But I know of no data to support this.
There are 2 excellent articles addressing whether a patient with completed MI should undergo PCI at all (vs. medical therapy alone), but none addressing this situation.
Schomig et al. published this in JAMA in 2005:
Data presented shows benefit of PCI (vs. medical therapy alone) for patients who present between 12-48 hours after STEMI if there was persistent STE, or simply new Q-waves, even in the absence of pain. But they did not assess the urgency of PCI.
Hochman et al. published the Occluded Arteries Trial (in the New England Journal).
In this article, they assessed arteries occluded for 3 days or more, and found that PCI resulted in worse outcomes than medical therapy.
The question this student posed was slightly different: beyond 12 hours, is emergent PCI better than delayed PCI (both groups getting PCI).
ACC/AHA 2013 STEMI guidelines say this:
CLASS IIa
Primary PCI is reasonable in patients with STEMI if there is clinical and/or ECG evidence of ongoing ischemia between 12 and 24 hours after symptom onset (94,95). (Level of Evidence: B). This means if there is chest pain, persistent ST elevation, or especially upright T-waves.
But the ACC/AHA guidelines do NOT address the timing (emergent vs. urgent) and they reference two studies, one of which is the Schomig article above, and the other of which also does not address emergent vs. urgent PCI.
94. Schömig A, Mehilli J, Antoniucci D, et al. Mechanical reperfusion in
patients with acute myocardial infarction presenting more than 12 hours
from symptom onset: a randomized controlled trial. JAMA. 2005;293:
2865–72.
95. Gierlotka M, Gasior M, Wilczek K, et al. Reperfusion by primarypercutaneous coronary intervention in patients with ST-segment elevationmyocardial infarction within 12 to 24 hours of the onset ofsymptoms (from a prospective national observational study [PL-ACS]).
Am J Cardiol. 2011;107:501–8.
Learning Points
1. I think if there is ongoing pain or ST Elevation, it is wise to go emergently to the cath lab to save any remaining viable myocardium. Randomized data on this is lacking. Probably, most researchers would be reluctant to test such management. Similarly, no one has ever conducted a randomized trial of emergent vs. delayed PCI for NonSTEMI with refractory (continued) symptoms.
2. PCI at some point within the first 12-48 hours of STEMI is definitely indicated.
Dr. Goldsmith of our Cardiology Department added his opinion in an email:
This
is a gray zone. Apropos of your general thinking that we should act to
make a clinical difference and not just on the basis of guidelines (!)
the issue of
timing here relates to how much salvage is likely. Points in favor of
going now: the relatively low trop on presentation (suggests possible
opening/closing of an
artery) with pain. If the trop had been 20 I probably would not have
gone…..pain and ST elev are problematic guides because both can
persist for many hours after there
is no chance of successful reperfusion (MI pain in the old days
required morphine for 24 hours, usually, as I remember from my
residency!). So these are
tough, and as you say there is no firm guidance. The low trop with a
rise suggest a new event or recurrent event to me, rather than a done
deal, so I probably would
have argued for earlier study knowing it might or might not help but
would not likely hurt. Perfect Pathway B case, by the way!