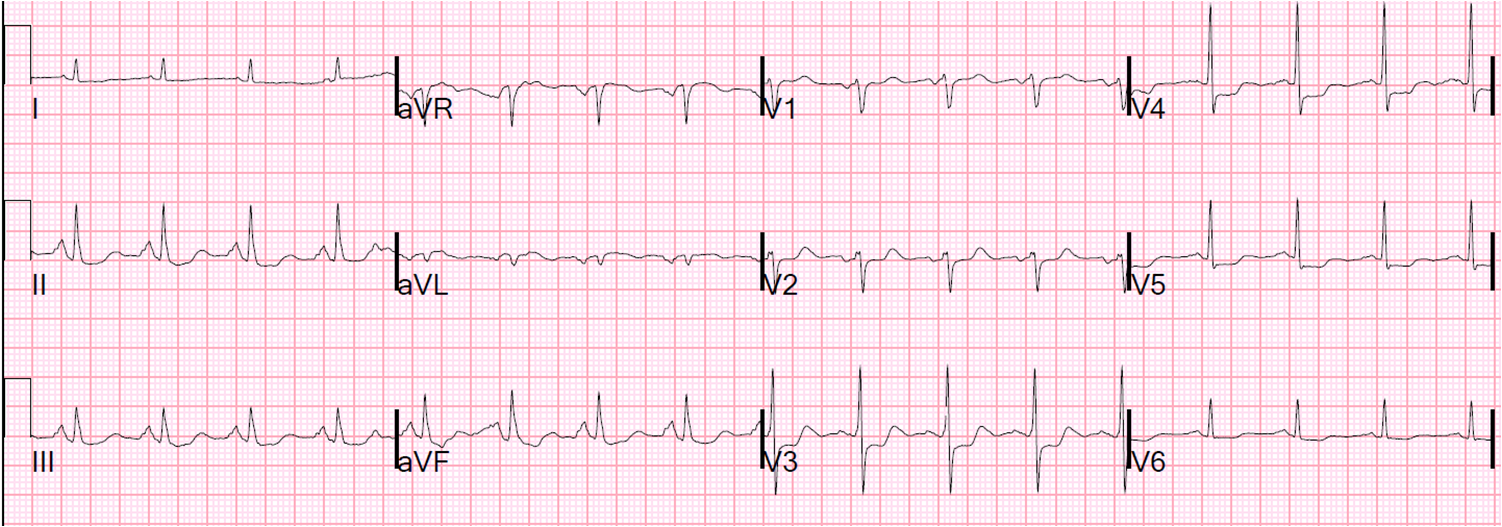
An otherwise healthy middle aged smoker complained of sudden left trapezius pain. He then began to fell very dizzy. He also had some vague left sided chest pain. His prehospital ECG was identical to the first ED ECG:
 |
| There is minimal ST elevation in inferior leads. What caught my eye was the T-wave inversion and minimal ST depression in aVL. This should always make you scrutinize the inferior leads for signs of inferior MI, and record serial ECGs. However, to my eye, inferior ST-T complexes did not appear to show MI. |
The patient’s symptoms were rather atypical, and because of this and the benign appearing inferior leads, I thought that the ST depression and T-wave inversion in aVL might not be pathologic. I signed the patient out to the next team with a plan to get serial ECGs and troponins, and manage according to the results.
The patient received NTG without change in his pain.
Another ECG was recorded shortly after the first and was identical.
The initial troponin I returned at 0.018 ng/mL (normal up to 0.030).
The second trop returned at 0.28 ng/mL (positive). The patient’s pain had not entirely resolved, but was at 3/10.
Persistent pain with objective evidence of MI is reason for aggressive management.
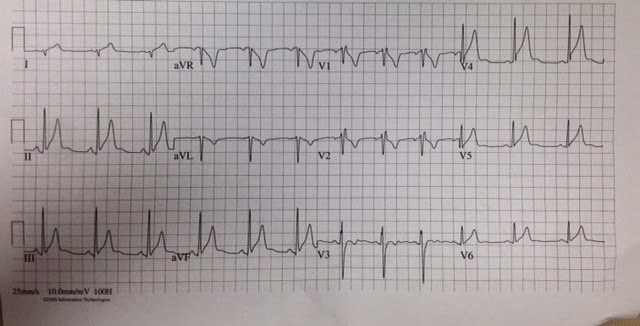
Another ECG was recorded:
 |
| There are some subtle, nondiagnostic differences in the inferior T-waves, which are now smaller. There are no unequivocal signs of coronary occlusion. The ST segments and T-waves are dynamic. |
He was started on antiplatelet and antithrombotic therapy.
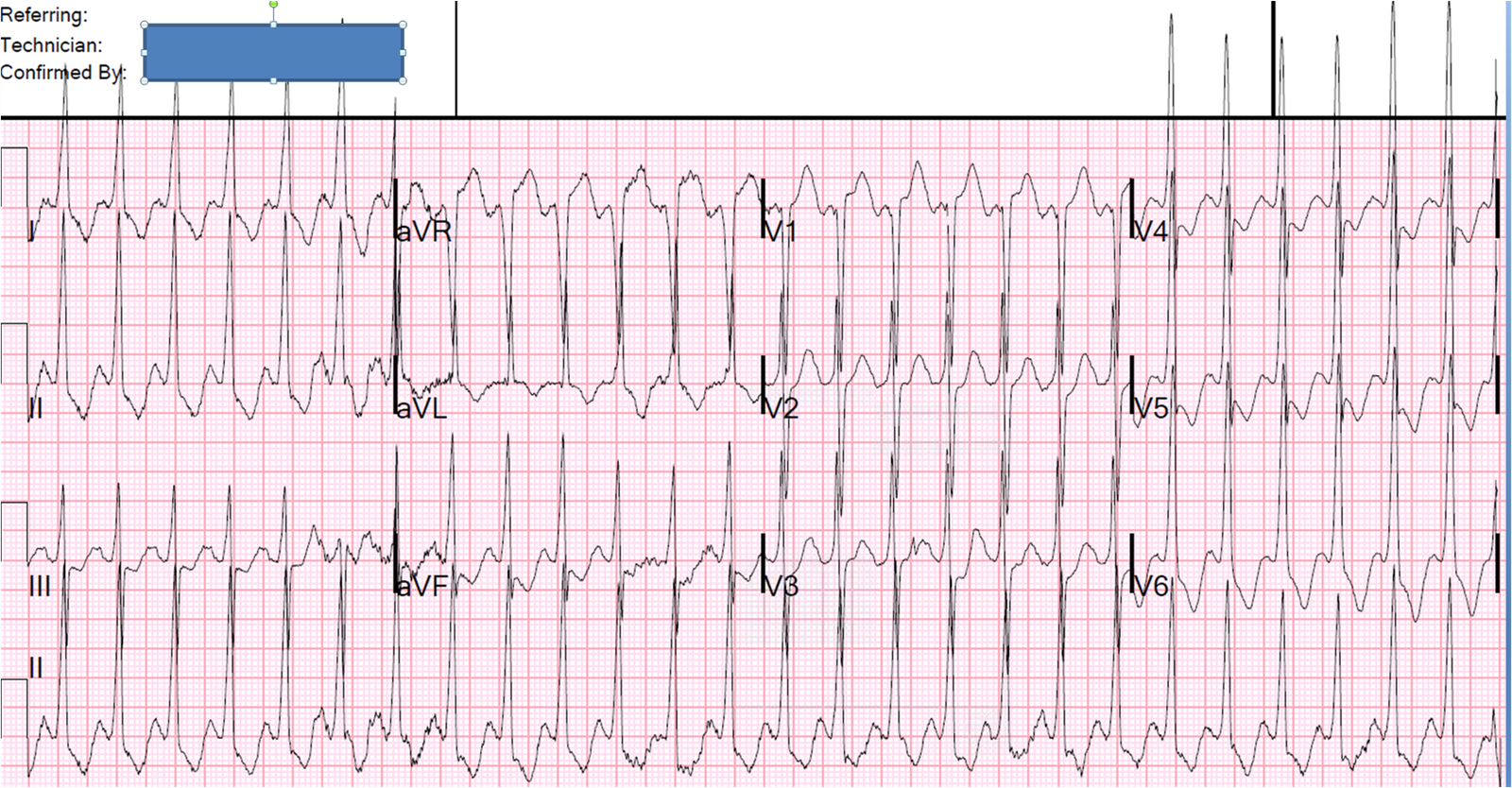
Suddenly, the patient developed sinus brady at a rate of 30, and had a 4 beat run of VT. He was hypotensive. The bradycardia and hypotension responded to atropine.
A bedside echo showed probable inferior wall motion abnormality.
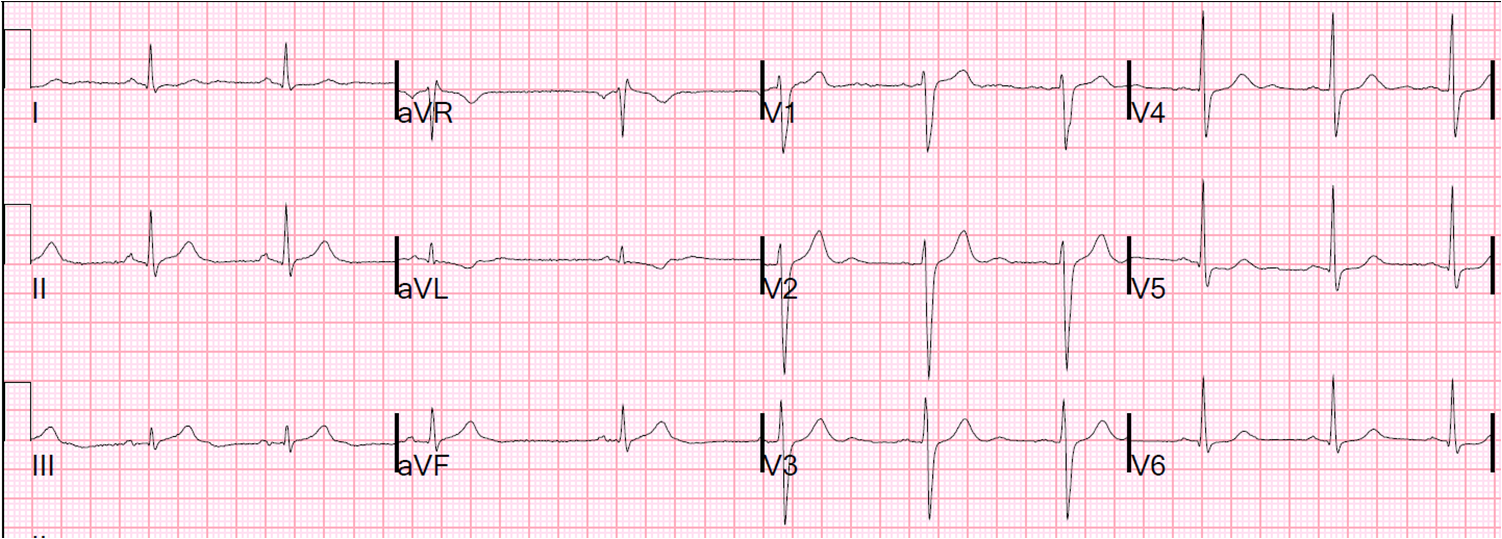
Another ECG was recorded:
 |
| Sinus bradycardia. Now the ST depression and T-wave inversion in aVL is resolved. The inferior ST segments are completely isoelectric. The inferior T-waves are smaller. There is new T-wave inversion in III and aVF. |
These are all signs of reperfusion, and indicate that the subtle findings of the first ECGs (minimal ST elevation, T-waves, ST depression and T-wave inversion in aVL) were all due to ischemia.
He was taken to the cath lab and found to have a severe 90% thrombotic lesion of the proximal to mid RCA.
In our study of inferior STEMI vs. non-MI causes of inferior ST elevation, any ST depression in aVL was almost perfectly diagnostic (sensitive and specific) for inferior MI.
Awareness of this finding allowed for vigilant observation and serial ECGs even in the absence of a typical history.