Written by Magnus Nossen
Today’s patient is a 60-something male with a history of atrial fibrillation managed with a rhythm control strategy (metoprolol and flecainide). He is otherwise healthy and physically active. Previous echocardiography had been unremarkable with only mild mitral regurgitation noted. On the day of presentation, he experienced sudden weakness, dizziness and a syncopal episode while shoveling snow. After regaining consciousness, he quickly had a second syncopal episode. Bystanders contacted EMS, and on EMS arrival the patient was awake and alert, reporting no chest pain. The patient was deemed stable by the paramedics who arrived at the scene. The initial ECG obtained is shown below.
What is your interpretation and how would you manage this patient?
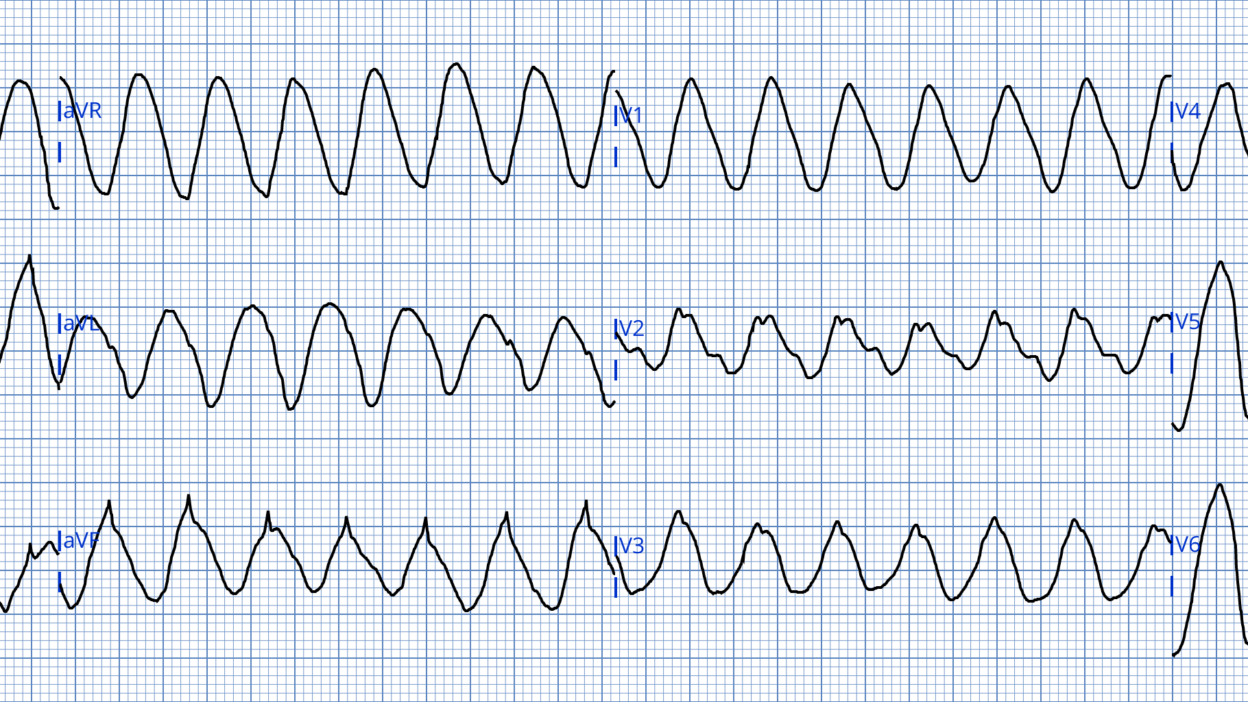
ECG #1 recorded by EMS
This ECG shows a wide complex tachycardia. RR intervals measure 345ms which gives a ventricular rate of about 175 beats per minute.
Medics at the scene recorded BP of 100 mmHg systolic and O2 saturations in the mid 90s at the same time ECG #1 was recorded. After consulting with the internist at the local hospital it was decided to give amiodarone 300mg bolus while transporting the patient to the nearby ED. Following amiodarone administration the heart rate normalized.
Smith: Is this change a result of amiodarone? Or is this coincidence? This morphology is a sine wave. In my opinion, amiodarone is not the answer. I would be worried about very wide QRS due to either flecainide or from Hyperkalemia. Immediate high dose calcium administration would be my management strategy, and would be appropriate for either etiology. VT from either of these etologies is also possible, so if calcium did not work, I would try cardioversion.
Magnus continues: I would say that this patient is not stable. Management with sedation and urgent cardioversion would have been another option as this patient has had two syncopal episodes and has an ongoing WCT.
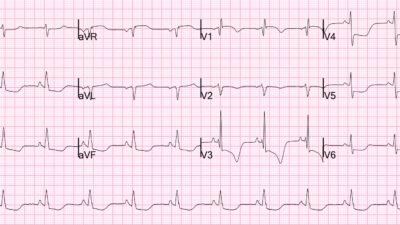
Transport to the ED was uneventful. The below ECG was recorded after first the evaluation in the ED, about 30 minutes after administration of amiodarone and achieved rate control.
ECG #2 recorded in the ED
Now the ECG shows an atrial arrhythmia with a controlled ventricular rate. The arrhythmia resembles but is not completely consistent with atrial flutter. The rhythm appears to be flutter in lead III, but regularly occurring flutter waves are not seen in leads V1-V2 — so this is likely some sort of transitional rhythm between atrial flutter and atrial fibrillation or vice versa. There are no clear signs of ischemia and no pathologic Q-waves. Non-specific ST-segment changes are noted in many leads. These changes are the result of superimposed “flutter” waves.
Case continuation: On arrival BP was 185/100. Heart rate was about 80 bpm with O2 saturation in the high 90s. No more WCT was observed in the ED. The prehospital ECG was interpreted as showing ventricular tachycardia and the patient was admitted to cardiology for further diagnostic investigations. A transthoracic echocardiogram was performed which showed mild to moderate MR, but no WMA, chamber enlargement or other pathologic findings. Cardiac MRi was normal ruling out any previous MI or myocardial fibrosis. A coronary angiogram was also done showing completely normal coronary arteries.
What do you consider the most likely cause of this patient’s WCT?
I was not directly involved with patient care. I did, however, see the prehospital ECG on the day of admission. I did not consider V-tach as the most likely diagnosis. Why do I say this? There are several reasons. Despite most wide complex tachycardias being VT in this patient age group, we know that this patient has a normal echocardiogram and is on medical treatment for A-fib. The QRS complexes in ECG #1 are very wide and in many leads show a sine-wave pattern! I measure the QRS duration at 225ms. A QRS this wide is rare in VT. It would be even rarer in a patient with a normal systolic function on echo and no known chamber dilatation.
Below I have reproduced leads V1-V3 from the original ECG. The original ECG was recorded with a paper speed of 50mm/second.
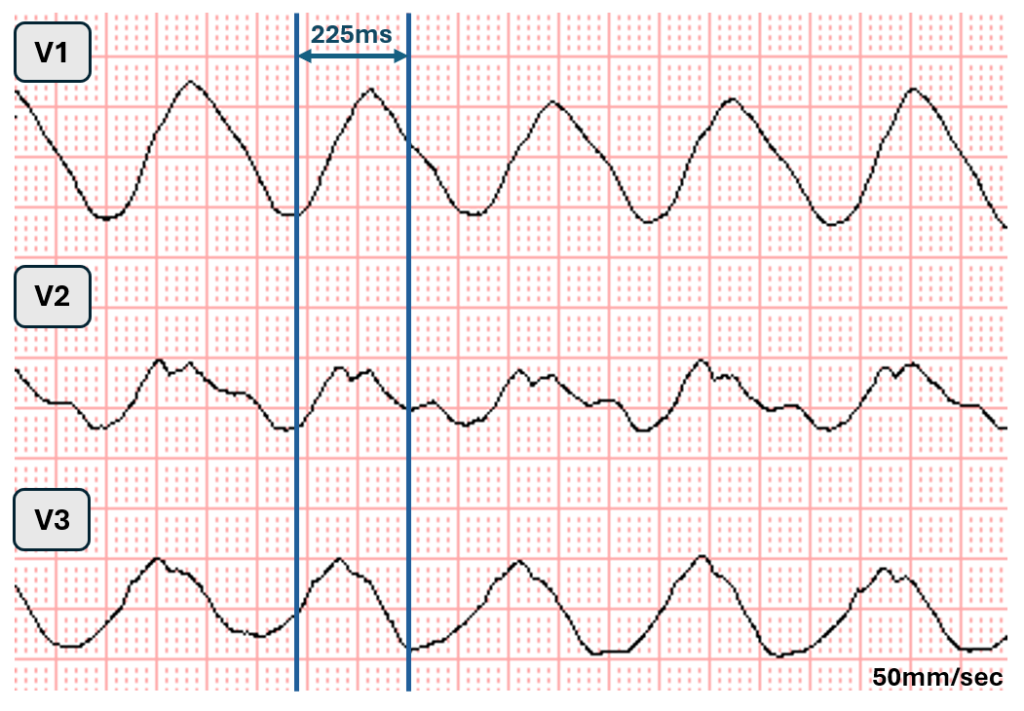
In the above excerpt showing right precordial leads, I admit it is very difficult to determine QRS onset and termination precisely. I think it is “easiest” to assess the beginning and end of the QRS in lead V2. Clearly the QRS duration is well above 200ms, I measure it at 225ms.
Whenever you find it hard to determine QRS onset and termination and the QRS is very wide (>180ms) you always need to think of sodium channel blocking effect.
The patient was prescribed flecainide (100mg) twice daily along with a low dose beta blocker. Flecainide can convert atrial fibrillation to atrial flutter and also markedly slow the flutter rate. This patient developed symptoms during physical exertion. This is characteristic of 1:1 atrial flutter as an increase in adrenergic tone will enhance AV nodal conduction making 1:1 conduction more likely to occur. This patient was perscribed 25mg metoprolol slow release once daily. Sometimes «low-dose» beta-blocker is insufficient to prevent 1:1 AV conduction during high adrenergic state as was clearly the case in today’s patient!
Flecainide exhibits use-dependent properties, meaning its effects — and potential toxicity are influenced by heart rate. The faster the heart rate, the stronger the sodium channel blocking effect becomes. This explains why tachyarrhythmias in patients treated with flecainide can present with markedly widened and bizarre looking QRS complexes. This also explains why ECG # 2 has a normal QRS duration. Amiodarone blocked the AV node sufficiently to control the ventricular rate. As the ventricular rate dropped the use-dependent sodium blocking effect lessened and the QRS narrowed.
Not uncommonly sodium channel blocking effect will present with “Brugada-like morphology” in leads V1-V2 which we also see in today’s case. (ECG #2 has some Brugada-like features)
After an extensive work-up was performed, it was concluded that this WCT was due to 1:1 atrial flutter with flecainide use-dependent properties accounting for the extremely wide and bizarre QRS complexes. Ablation for atrial flutter was performed and flecainide was discontinued. Long term follow up is unavailable.
Addendum to today’s case
Is the use-dependent effect of flecainide clinically relevant?
Yes!
Below are two rhythm strips from a DIFFERENT patient. This patient in his 70s was receiving flecainide for atrial fibrillation rhythm control. The recordings below, obtained approximately 60 minutes apart, illustrate how the use-dependent properties of flecainide during tachycardia can significantly alter QRS duration and morphology.
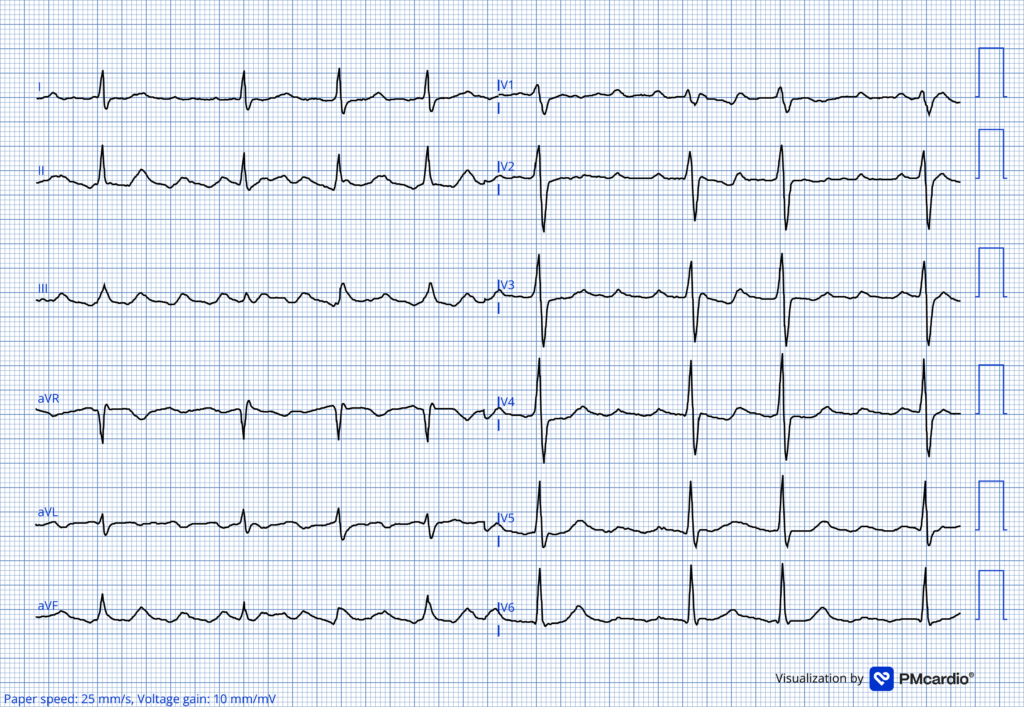
Rhythm strip #1 at time zero
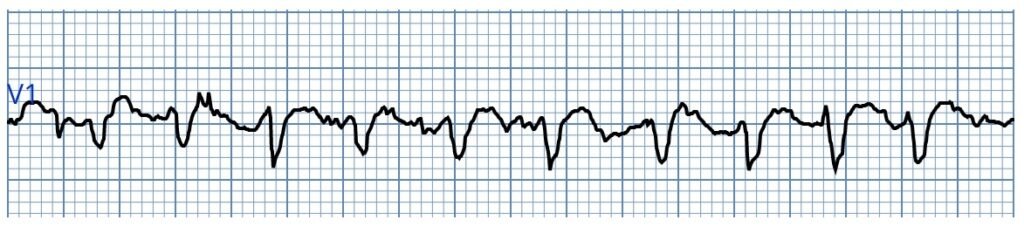
Initial rhythm strip from a patient with A-fib and RVR. This lead V1 rhythm strip demonstrates a mild sodium channel–blocking effect with slight QRS prolongation
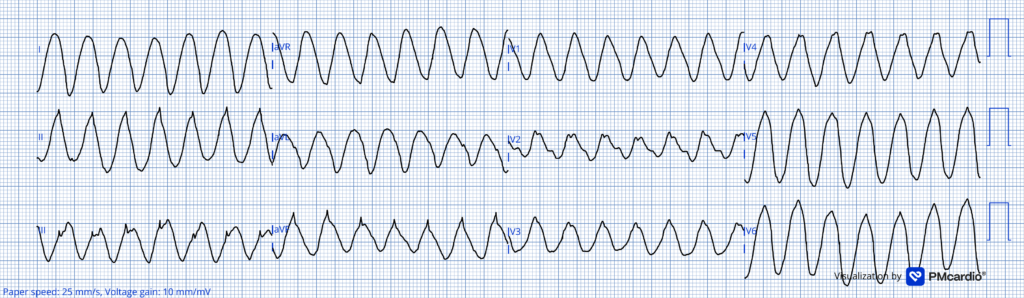
Rhythm strip #2 at 60 minutes
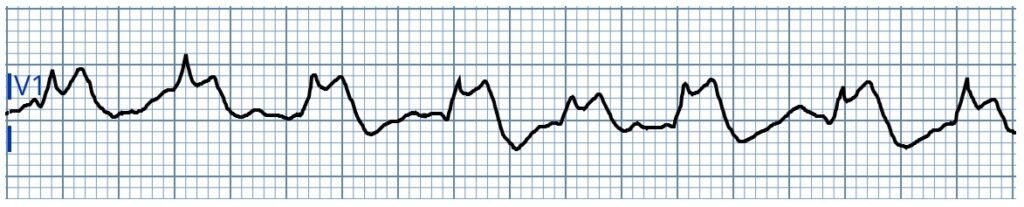
Repeat rhythm strip from the same patient approximately 60 minutes after the first recording. This tracing shows a markedly abnormal QRS appearance, exhibiting an atypical Brugada-like pattern provoked by the use-dependent effect of flecainide! Shortly after this second ECG was obtained, the patient experienced V-fib arrest. This case is presented in detail HERE.
For more cases on flecaininde see this case, this case and this case.
Learning points
- Whenever the QRS complex becomes markedly widened and or bizarre in appearence, consider a sodium channel–blocking effect, as seen with flecainide, hyperkalemia, or tricyclic antidepressant toxicity.
- In a patient with atrial fibrillation treated with flecainide, always consider 1:1 atrial flutter as a potential cause of a wide-complex tachycardia.
- It is important to remember that flecainide exhibits use-dependent properties, with stronger effects and a higher risk of adverse reactions at faster heart rates.
- Use dependency of flecainide occurs in atrial and ventricular myocardium. The effect on ventricular myocardioum is the most clinically relevant as this may lead to ventricular fibrillation as shown in the case referenced in the addendum.
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/23/2026):
Important case by Dr. Nossen — in that it highlights a series of learning points regarding assessment of the regular WCT (Wide-Complex Tachycardia) rhythm in a patient on Flecainide.
- As per Dr. Nossen — It could be easy to overlook the findings in ECG #1 (recorded by EMS) that: i) The QRS is very wide! — and, ii) QRS morphology for monomorphic VT at the fast but not excessively fast rate of ~170/minute should not manifest this bizarre of a QRS morphology that resembles a sine wave appearance without clear distinction of the onset and offset of each QRS complex in ECG #1.
- Instead — some toxicity (ie, Hyperkalemia, sodium-channel blockade, etc.) should immediately be suspected on seeing ECG #1.
= = =
Flecainide Toxicity:
As per My Comment in the May 21, 2023 post — Flecainide toxicity is a relatively uncommon — but extremely important condition to recognize. The mechanism of this toxicity is multifactorial. Potential for widespread adverse clinical effects is great. The mechanism and resultant clinical effects include:
- Sodium Channel Blockade — which inhibits fast sodium channels, leading to reduced conduction velocity with significant (if not marked) QRS widening and PR interval prolongation.
- Slowing of Calcium and Potassium Channels — with resultant depressed contractility (negative inotropic effect) and hypotension.
- Rate-Dependency (as emphasized above by Dr. Nossen): Because drug binding increases at faster heart rates — toxicity (especially QRS widening) worsens with tachycardia (as apparently occurred in today’s case with development of 1:1 AFlutter).
Bottom Line: In addition to the negative inotropic and hypotensive effects of Flecainide toxicity — there is depression of all major conduction pathways (ie, in the AV Node; His-Purkinje system, and in the ventricles). This may result in a series of conduction disorders including various forms of AV block; bundle branch blocks; impaired pacemaker function.
- The QRS may be markedly widened with a bizarre morphology (as seen in ECG #1 of today’s case).
- Lethal arrhythmias may be a terminal event (VT/VFib; Asystole).
- Overall — Flecainide Toxicity is suggested when: i) There is ≥50% increase in QRS duration (typically producing a QRS ≥0.18 second); — and/or, ii) A ≥30% increase in PR interval duration (typically to a PR ≥0.26 second). The QTc may also be increased (though much of this effect is the result of QRS rather than QT prolongation).
= = =
Management Considerations:
Today’s patient was treated with Amiodarone — after which the heart rate slowed and the QRS complex normalized in both width and morphology (as shown in ECG #2). But if clinical manifestations of Flecainide toxicity persisted:
- Sodium Bicarbonate — has been the treatment of choice (Bicarb provides a high sodium load that competitively displaces Flecainide from sodium channels — thereby raising blood pH, which reduces the active, ionized fraction of Flecainide).
- Caution: Use of conventional antiarrhythmic drugs may be ineffective or even exacerbate Flecainide-induced arrhythmias by worsening sodium channel blockade (Stolear et al — Cureus 16(6),e62923- 2024). Amiodarone may further aggravate Flecainide toxicity by inhibiting CYP450 2D6, the isoenzyme responsible for the metabolism of Flecainide (Drugs.com).
- ILE (Intravenous Lipid Emulsion) — another proposed treatment — beyond the scope of this ECG Blog (ILE acts as a “lipid sink” that attracts and isolates lipophilic drug in blood, thereby reducing binding to cardiac myocytes).
= = =
= = =