This 63 yo male with no cardiac history had 30 seconds of syncope. When he awoke, he complained of progressively worsening substernal chest pain associated with nausea and diaphoresis. He had 2 prehospital ECGs and 4 hospital ECGs before he was taken to cath. Here is the succession:
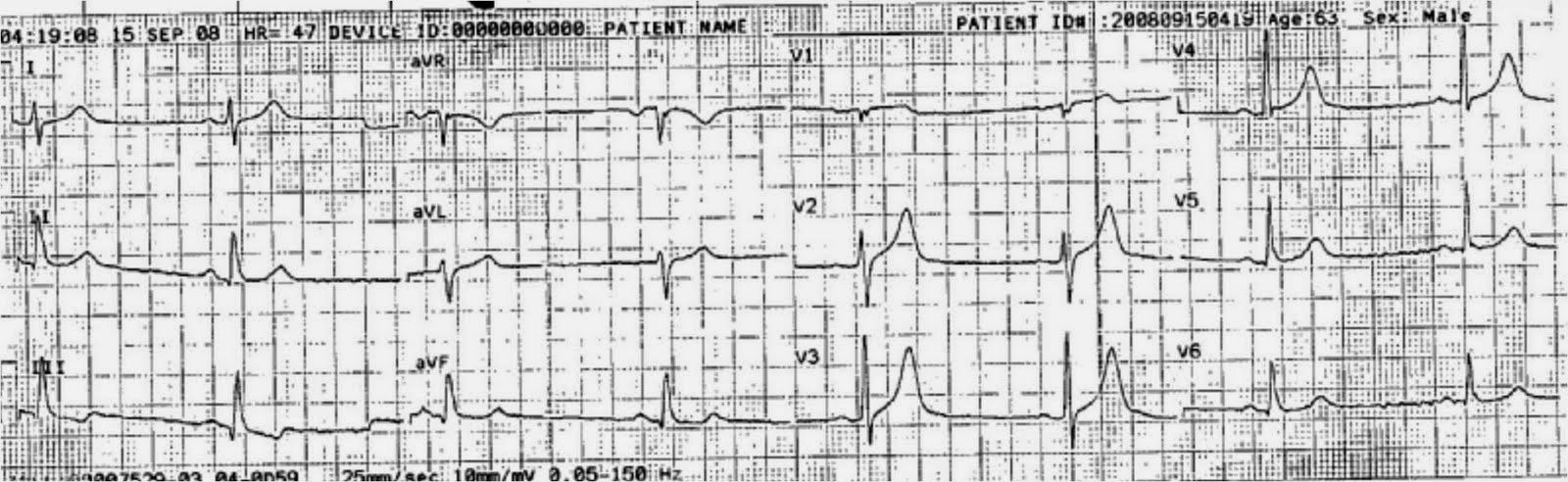 |
| Prehospital ECG with sinus bradycardia. There is ST elevation and tall T-waves that looks like early repolarization. The ST segment and T-wave in lead III should raise suspicions for LAD ischemia. |
 |
| First ED ECG 0349. There is an apparent junctional rhythm. The ST elevation is gone. The T-wave in lead V2 is no longer tall. Lead III still looks suspicious. LAD high grade ACS is certain with these changes. This was not appreciated. A pulmonary embolism workup was done. |
 |
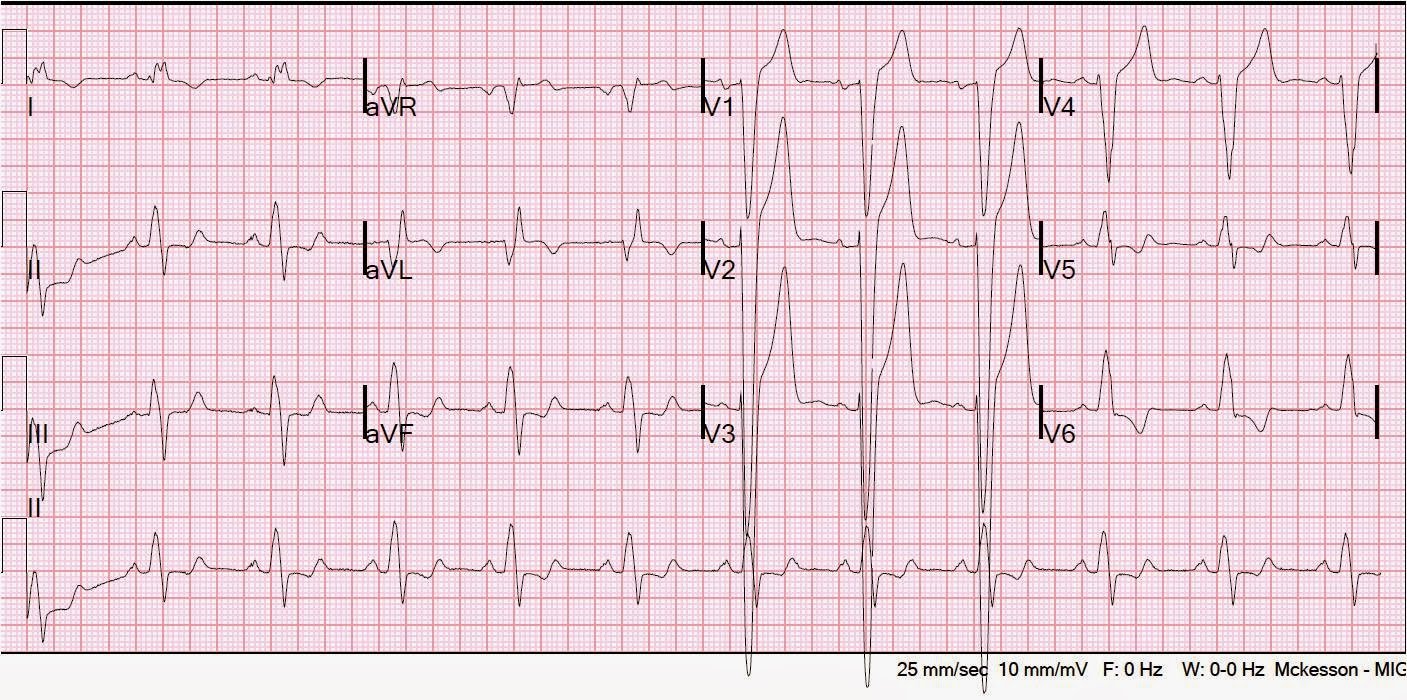
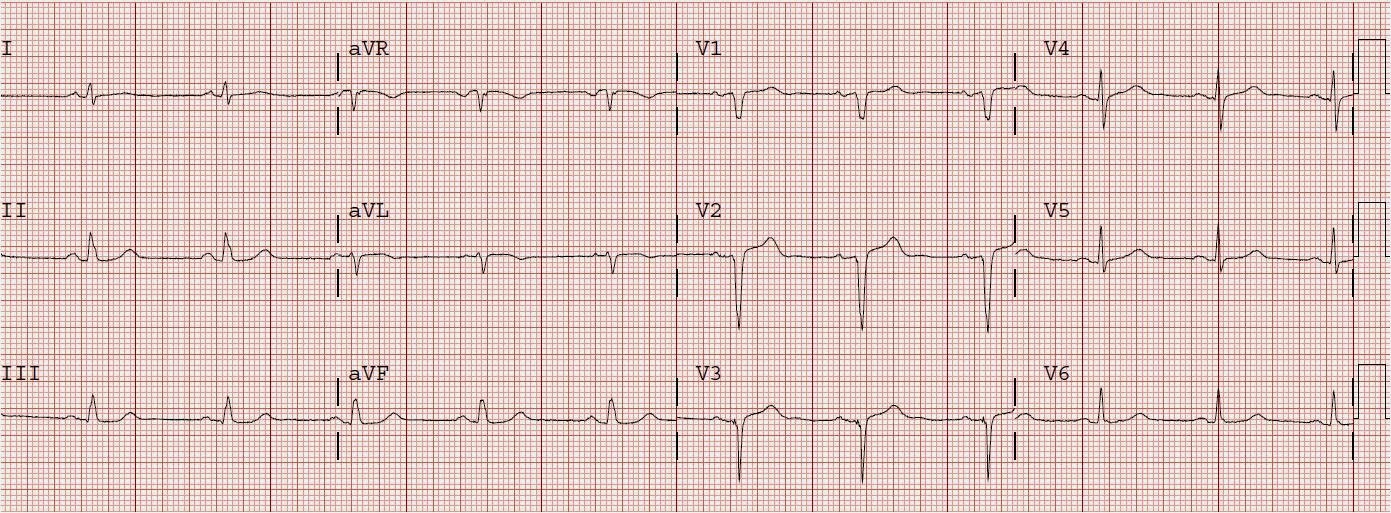
| Second ED ECG 0432. There is new ST depression in leads I, III, and V3-V6. V3, with a large T-wave and ST depression, is “A New Sign of LAD occlusion” de Winter et al. N Engl J Med 2008;359(19):2071. Still the cath lab was not activated. |
See this post for more of these T-waves: https://drsmithsecgblog.com/2009/02/hyperacute-t-waves.html
 |
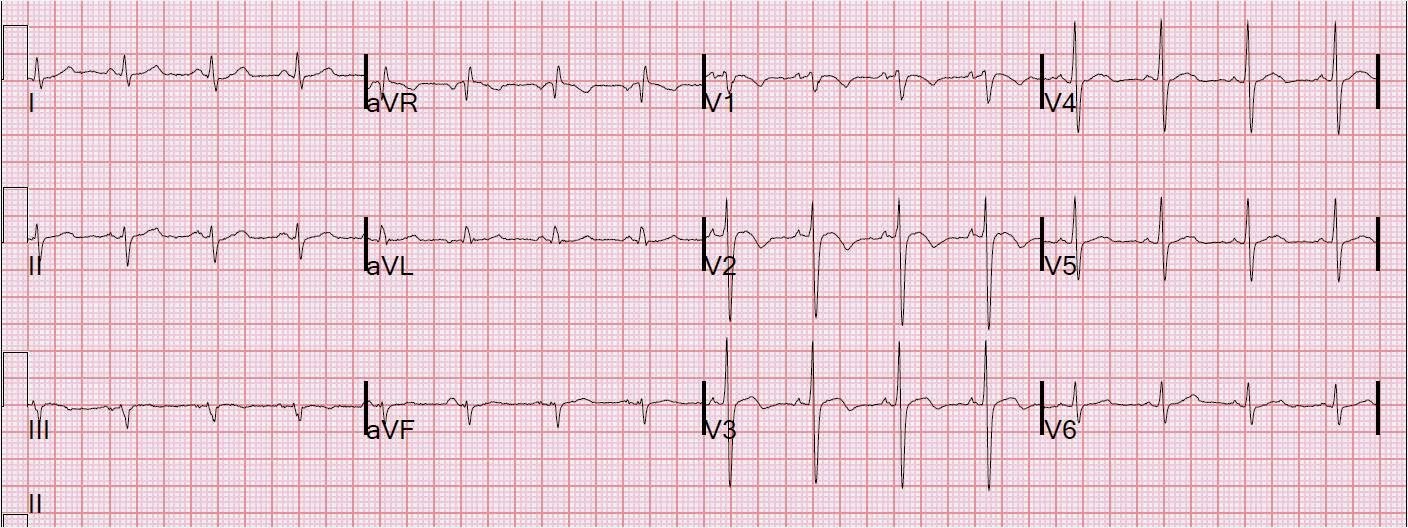
| 3rd ECG 0439. Hyperacute Ts and ST depression mostly resolved. The patient was admitted to cardiology. |
 |
| 4th ECG 0605. Recurrence in V3 of hyperacute T with ST depression |
At this point, the patient was taken for cath. He was found to have 100% LAD occlusion just after the D1 takeoff, but also had a severe 90% RCA co-culprit ruptured plaque.The LAD was getting some flow through right to left collaterals, which explains the subtlety of the ECG. Maximum troponin I was 36 ng/ml.
 |
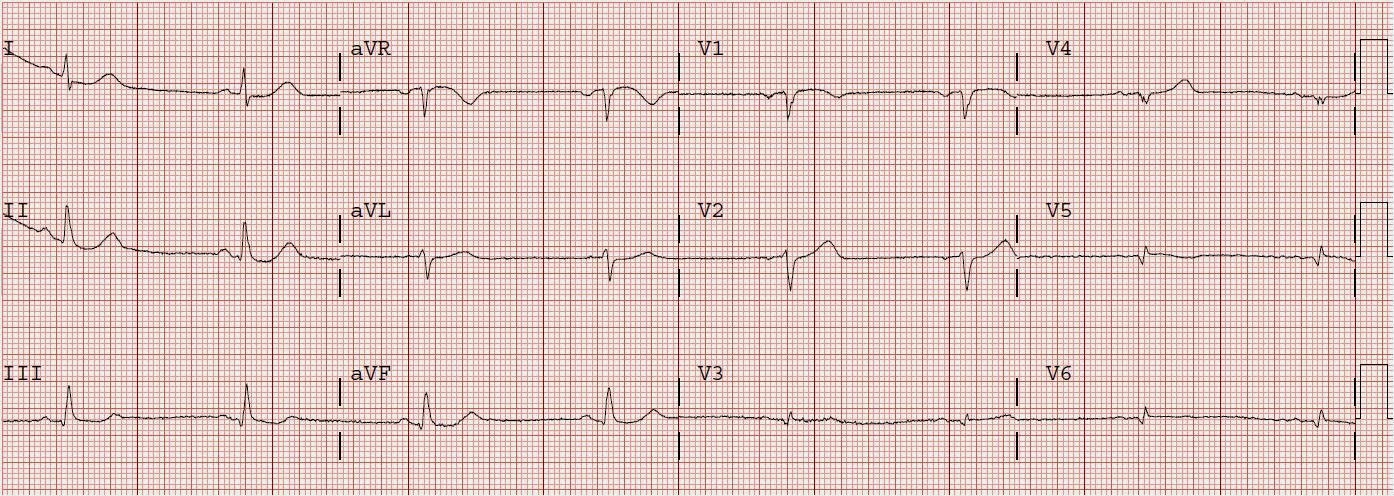
| After cath and PCI. The R-waves are gone. There are only QS-waves in V2 and V3. There is some persistent ST elevation. There is T-wave inversion in aVL. |
 |
| Next day ECG: T-waves are beginning to invert in V2 and V3 |
Although the peak troponin is not extremely high, the ECG would suggest that much of the anterior wall infarcted in spite of minimal ST elevation. In the de Winter’s study, they report that the ST depression followed by a large T-wave was persistent and did not develop into ST elevation. Whether this is true with all such patients is in doubt, as it requires ECGs to be done frequently.
Nevertheless, de Winter’s T-waves should trigger the cath lab.
And so should the Transient ST elevation seen on the prehospital ECG.