This patient was found with a bottle of alcohol and altered mental status. His breath alcohol was 0.259. Due to bradycardia, a 12-lead ECG was obtained:
 |
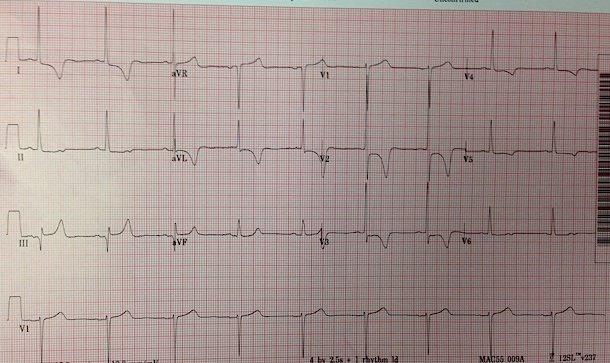
| There is atrial fibrillation at a rate of 54. The QRS is 166 ms. Why is it slow? What is the diagnosis? |
This is pathognomonic and you must recognize this! There is a wide QRS and peaked T-waves. In particular, notice how flat the ST segment is before it abruptly rises into the T-wave!
HyperKalemia was immediately recognized and the patient was given Calcium.
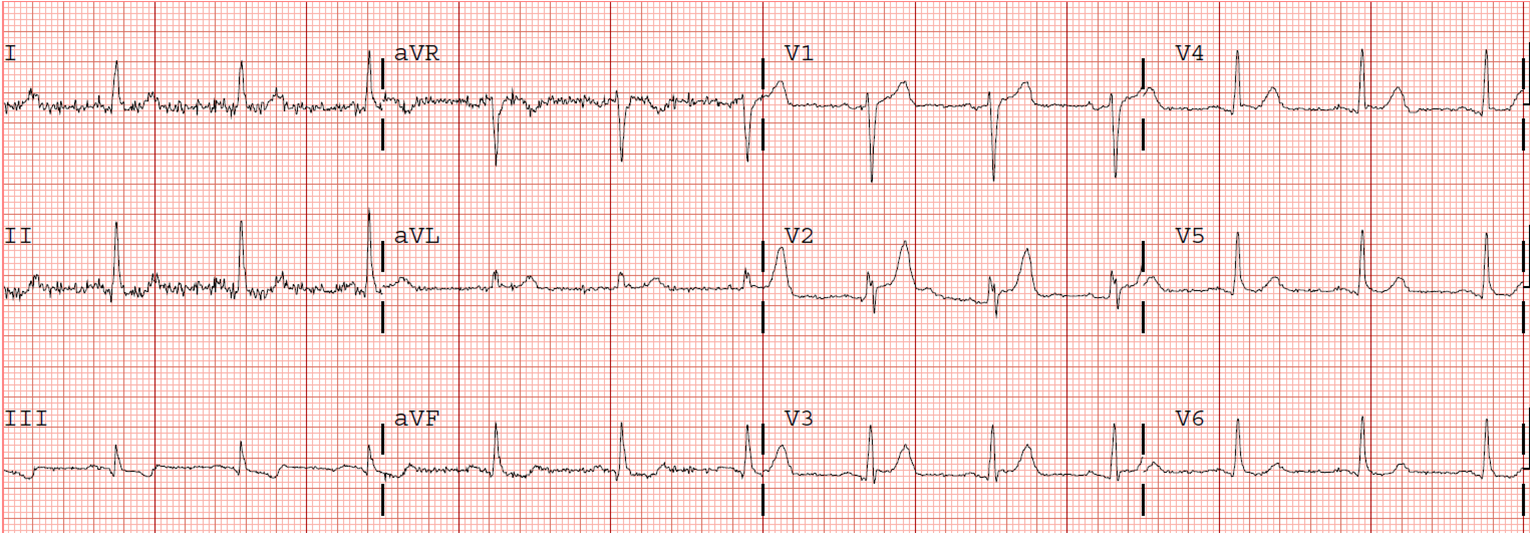
A followup ECG was obtained after Calcium:
 |
| The QRS is now 129 ms. |
The potassium returned at 7.8 mEq/L. His pH was 6.97. It was caused by new onset of acute renal failure.
This patient could easily have been just assumed to be intoxicated. He might have been brought to detox, or might have just been observed in the ED.
But because of bradycardia, a 12-lead was obtained, which gave the critical diagnosis.
Learning Points:
1. When a patient is bradycardic, especially if irregular, one must always think of hyperK and one must get a 12-lead ECG.
2. One must recognize this pattern as hyperK
3. Calcium’s effect is almost miraculous
4. Slow atrial fibrillation implies an sick AV node, or one affected by electrolytes, ischemia, or medications/drugs. Otherwise, the ventricular response should be fast.