We have completed and published the external validation of the Modified Sgarbossa Criteria for Diagnosis of Acute Coronary Occlusion in the Presence of Left Bundle Branch Block.
H. Pendell Meyers had just graduated from college when he took this project on. Now he is a 4th year student at Duke, interviewing for Emergency Medicine Residency Positions.
He did amazing work on this project.
Here is a link to the abstract:
http://www.sciencedirect.com/science/article/pii/S0002870315005918
A quick summary:
Sgarbossa criteria:
1. at least 1 mm of concordant ST elevation in at least one lead (5 points)
2. at least 1 mm of concordant ST depression in at least one of leads V1-V3 (3 points)
3. at least 5 mm of discordant ST elevation in at least one lead (2 points)
Weighted criteria (the actual Sgarboss criteria): At least 3 points required to make the diagnosis of acute MI. Thus, criterion 3 is not sufficient.
Unweighted criteria: any one of the above
Derived Smith-Modified Criteria, published in 2012 in Annals of EM (amazing work on this was done by Dr. Ken Dodd, who was a medical student at the time and is one of our emergency medicine/internal medicine residents now):
1. at least 1 mm of concordant ST elevation in at least one lead (5 points)
2. at least 1 mm of concordant ST depression in at least one of leads V1-V3 (3 points)
3. at least 1 mm of discordant ST elevation AND an ST elevation to S-wave ratio of at least 25% in at least one lead.
Validation Results:
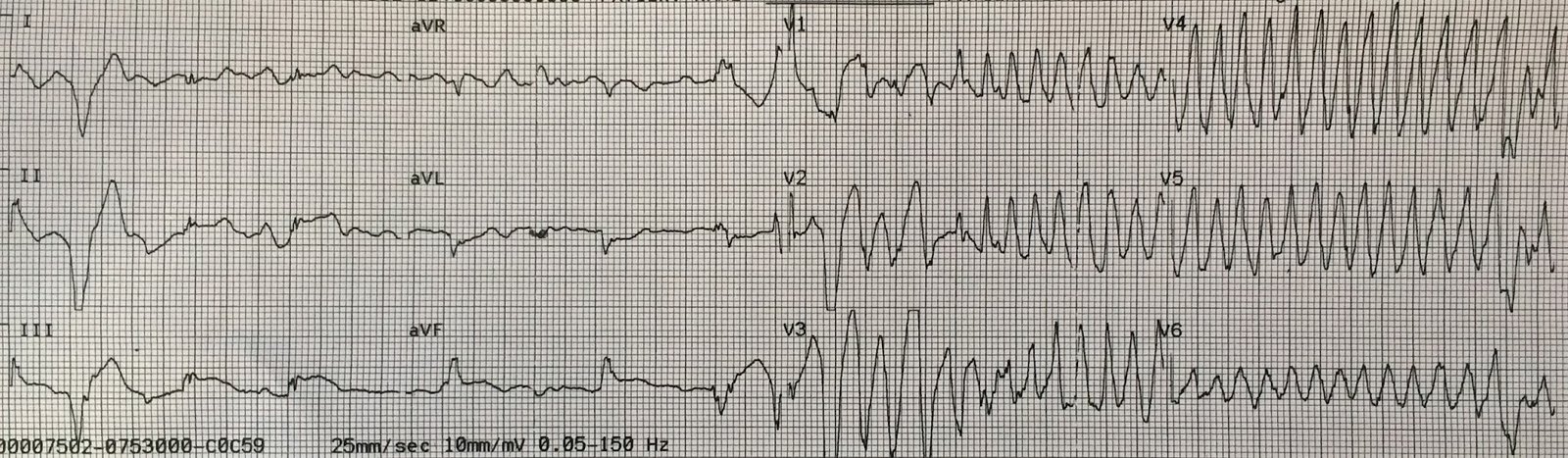
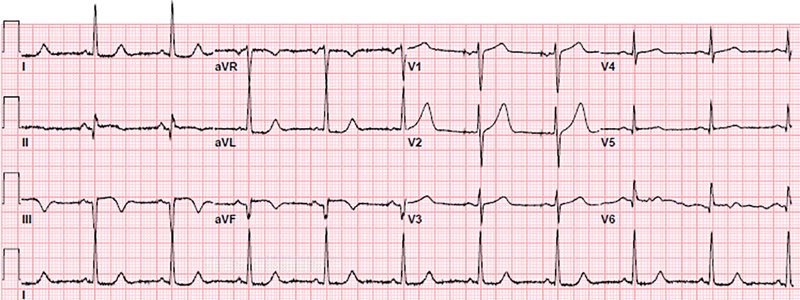
There were 45 patients with LBBB and acute coronary occlusion and 249 controls:
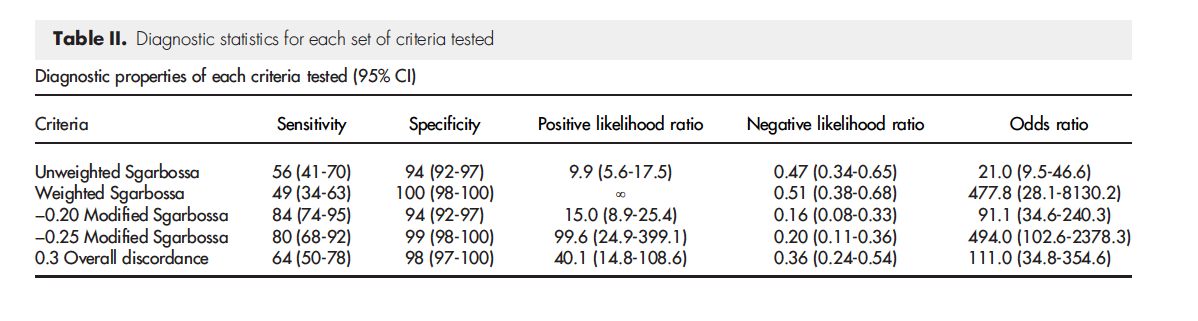 |
| The Modified Criteria (ST/S ratio of greater than or equal to 25%) was far more sensitive than either the weighted or unweighted Sgarbossa criteria |