A male in his 60’s called 911 for dizziness and chest pain, onset with exertion. He was pale and diaphoretic (in shock) with a thready radial pulse.
Here is his initial rhythm strip (it is not a full 10 seconds):
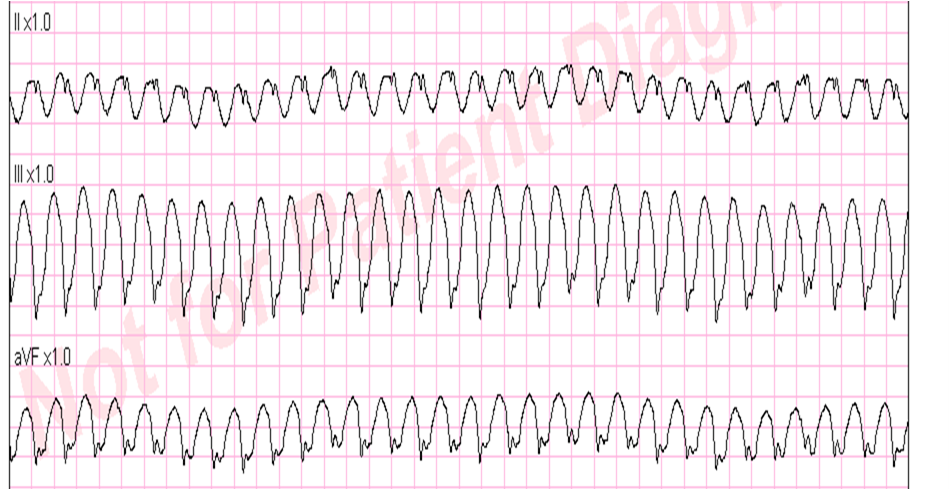 |
| Wide complex tachycardia, rate 235 |
 |
| This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such. |
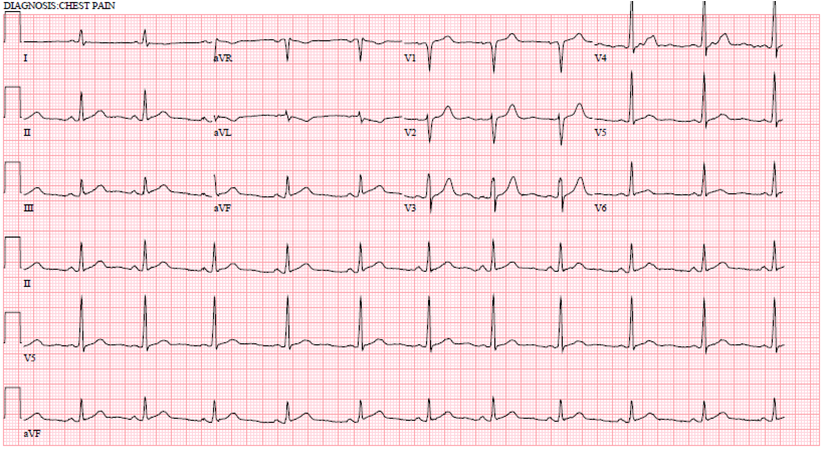
Here is the 12-lead:
By any analysis, it is most likely VT: There is slow depolarization of the initial deflections of the QRS. However, this is a very fast VT.
The patient should be safely sedated and electrically cardioverted.
The paramedic instead gave adenosine, which is not contraindicated, and will not harm a patient in VT. It is now part of the ACLS protocol.
If it is VT, as suspected, it will not work (RV outflow, adenosine sensitive VT is likely to respond, but this is NOT such a benign VT as it is too wide and does not have the right morphology).
If it is SVT with aberrancy, it is likely to work.
If it is AV reciprocating (antidromic WPW), adenosine is likely to work.
If it is slow Atrial flutter with 1:1 conduction, it should slow the conduction and reveal the flutter waves. This is the exact rate one expects with slow atrial flutter and it is why slow atrial flutter can be so dangerous: it conducts 1:1, with fast ventricular rates.
Here are the monitor leads during and after adenosine:
During adenosine:
 |
| Lead II is monitored. The rate starts at 222 with a wide complex. It is uncertain to me why the initial rate is slower than the rate above; it is clear though that it is the same rhythm because lead II has the same morphology. In the middle of the second strip, there is a minimal pause, after which the complexes are narrow, and after which there are visible flutter waves at a rate of 228. There is mostly 2:1 conduction, but some 1:1 |
After adenosine:
 |
| The strip continues: now the flutter waves are easily seen at a rate of 240 (almost exactly the same rate it started with) with 2:1 conduction and a relatively narrow complex QRS (less than 120 ms). |
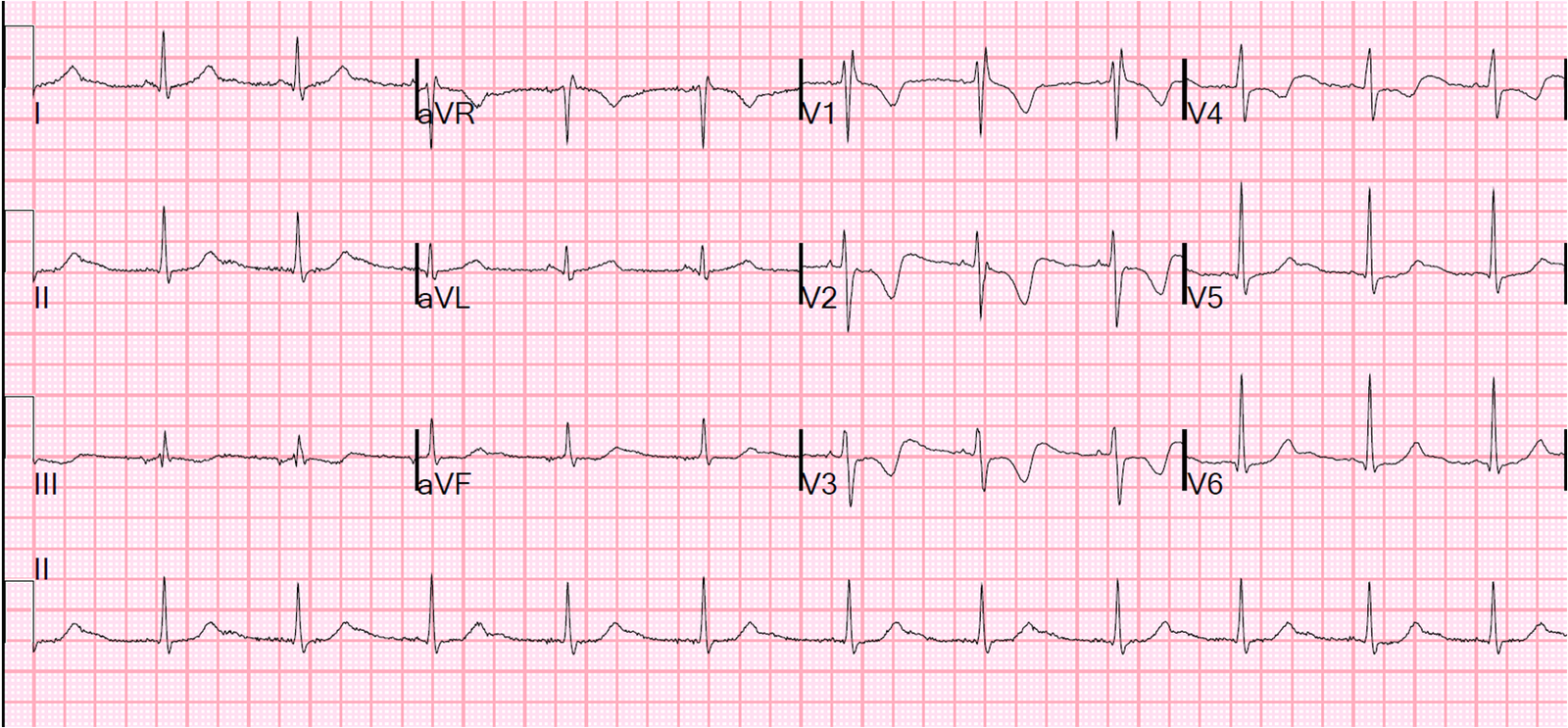
2 12-lead ECGs were recorded within the next 3 minutes:
 |
| Rate 118, flutter rate 236: One can see the flutter waves in lead II, and an upright P-wave in V1 confirms that this is flutter. Some of the ST depression is due to flutter waves, but there is also significant subendocardial “demand” ischemia. ACS is of course possible. |
 |
| Rate 120, flutter rate 240. Still more ST depression. |
So what happened?
One might speculate that the patient co-incidentally converted from VT to atrial flutter at the time of the adenosine. But I think that this atrial flutter was just slow enough to conduct through the AV node but too fast to use the conducting system, so if conducted through the ventricles VERY aberrantly and, the first time that there was AV conduction delay (2nd line of rhythm strip during adenosine), the conducting system recovered (was no longer refractory) and was able to conduct such that the QRS is a relatively narrow complex.
How do I know (or think I know) it was atrial flutter with aberrancy?
Because the rates before and after the change in conduction are nearly exactly the same. Again, see line 2 of rhythm strip during adenosine. It is clearly atrial flutter after, so it must have been atrial flutter before
Did adenosine convert anything?
No, but it appears to be associated here with a slight increase in atrial flutter rate and thus subsequent 2:1 conduction with slower ventricular response (atrial flutter 240, faster, but ventricle at 120, slower).
Learning points:
1. Sometimes it is better to be lucky than right.
2. Generally, adenosine is safe in VT
3. If it looks like VT, treat it like VT. Don’t count on being lucky.
4. Slow atrial flutter can produce VERY FAST ventricular rates.
5. Very fast ventricular rates may conduct very aberrantly and be very wide.
6. Sometimes what appears to unequivocally be VT is not
Comments appreciated.