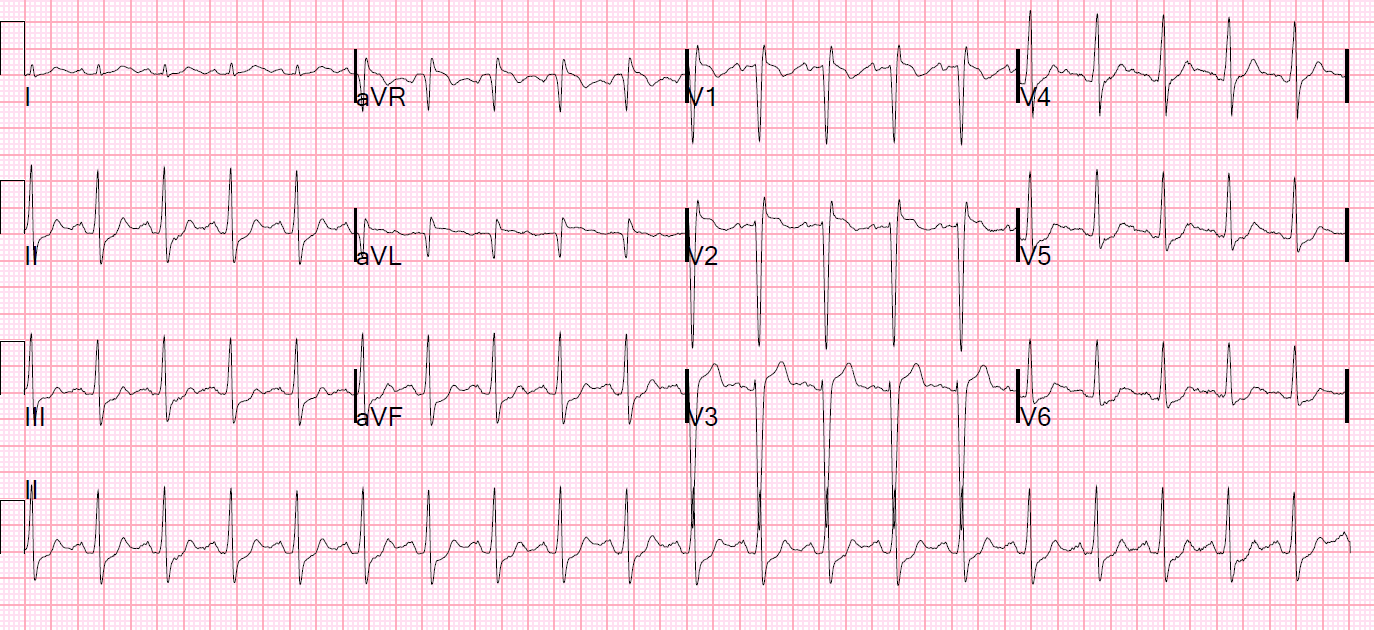
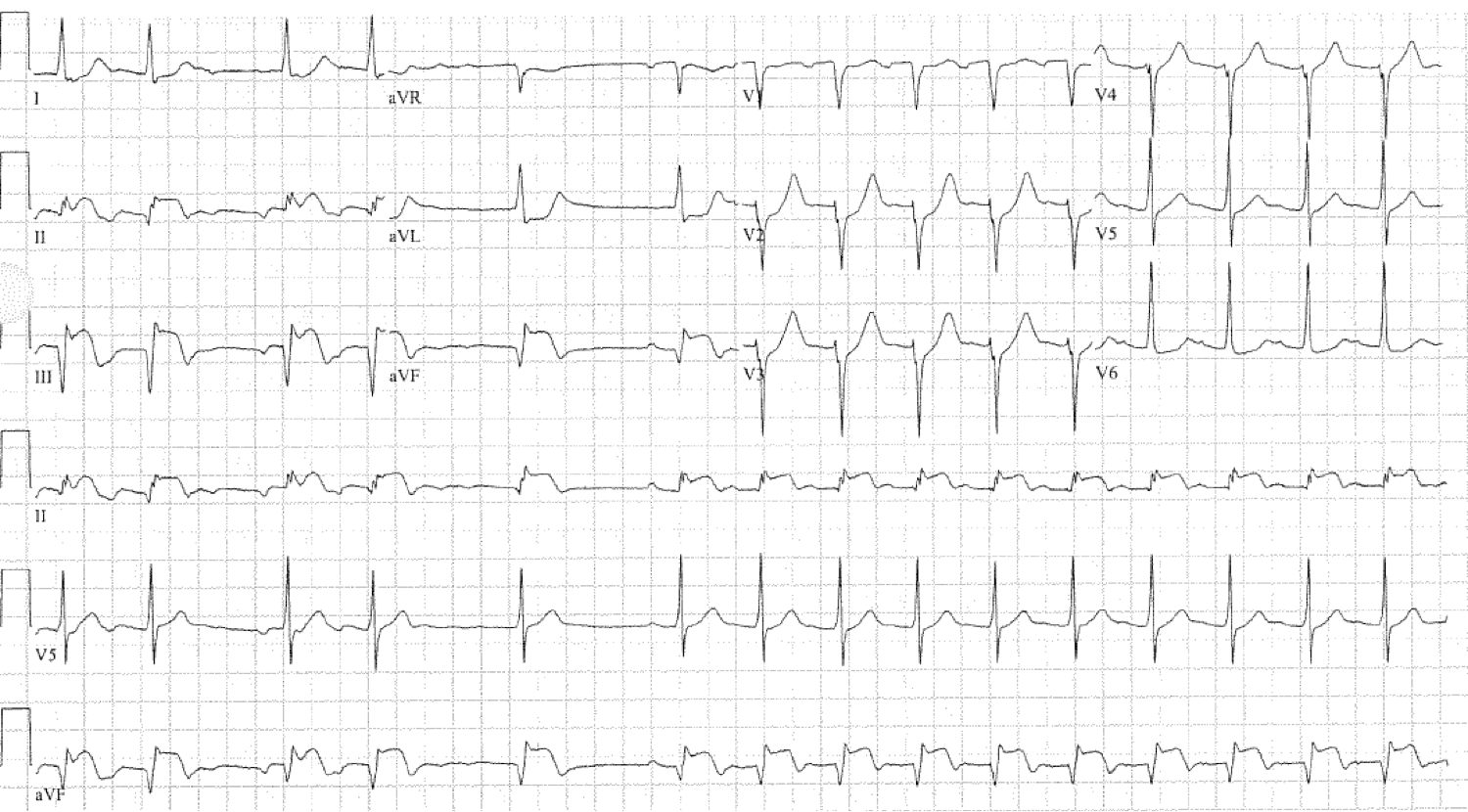
A patient presented with chest pain and had this ECG:
 |
| There is obvious ischemic ST elevation with reciprocal ST depression.
What is the culprit artery? |
A high lateral STEMI was diagnosed and the patient was taken to the cath lab.
The interventionalist was surprised to find that the infarct artery was the RCA.
This was sent to me for explanation. What is the explanation?
If you look at the QRS, you see that there are well formed R-waves in V5 and V6, but a Q-wave in aVL and very low voltage R-wave in lead I. All are lateral leads and usually have similar QRS findings (though not always because V5 and V6 are more inferior than I and aVL). The difference in this case is too large to be due to this normal variation.
So I stated that the leads were misplaced and to send me an ECG with the leads properly placed, if one was available.
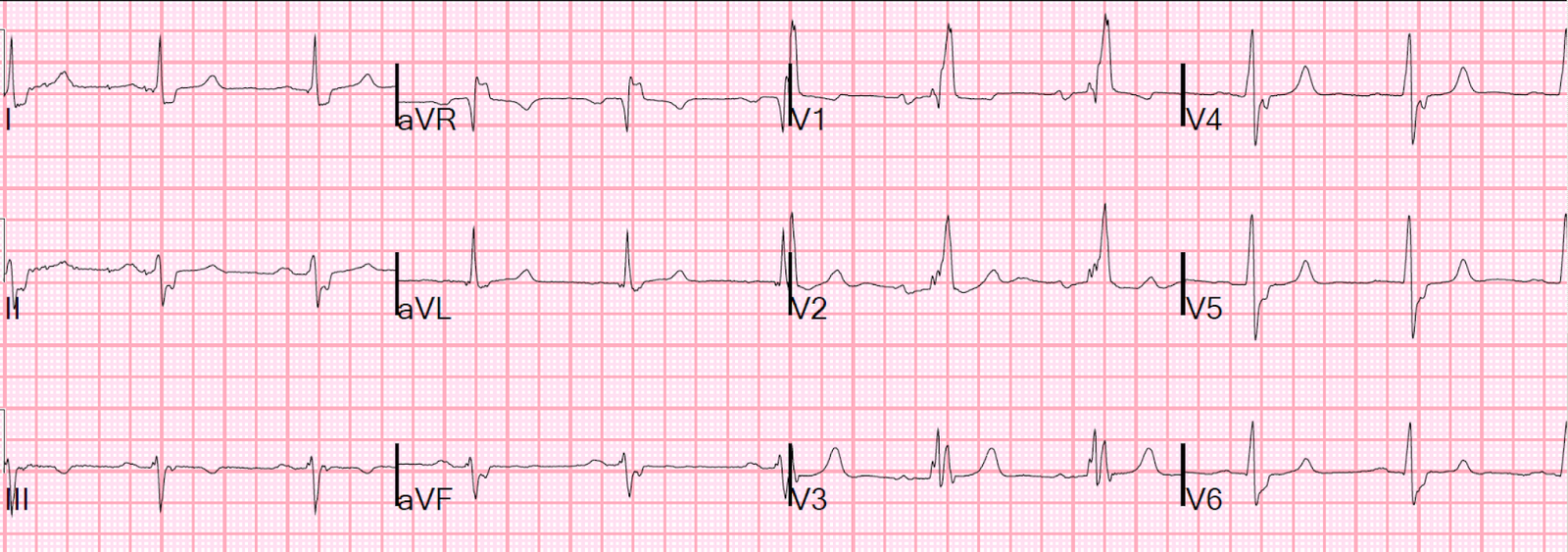
Fortunately, there had been a second ECG recorded slightly later. It was available and sent:
 |
| Now the R-wave is clearly positive in all lateral leads. Thus, in this ECG, leads were properly placed. And the ST elevation is inferior, with reciprocal ST depression in I and aVL. |
Learning Point:
1. Try to assess the QRS before assessing the ST segments and T-waves. Our eyes are always drawn to the ST segments first.
This is similar to proper technique of reading an X-Ray. One is always drawn to the pathology, or the pathology one is seeking. If you look elsewhere first to find any incidental or related findings, you will not forget to look for pathology. But if you look for pathology first, you will forget to scrutinize the remainder of the exam and will miss important findings.
This behavior also leads to the misdiagnosis of PseudoSTEMI patterns as STEMI patterns: many PseudoSTEMI patterns are abnormal repolarization (ST-T abnormalities) that are due to abnormal depolarization (abnormal QRS). If you look at the QRS first, you will not miss the LVH or RVH or bundle branch block or Brugada or hyperK. Then when you see the ST elevation you will be prepared to know that it could be secondary to an abnormal QRS (not primary due to ischemia).