======================================
MY Comment, by KEN GRAUER, MD (11/12/2019 — Updated on 10/29/2025):
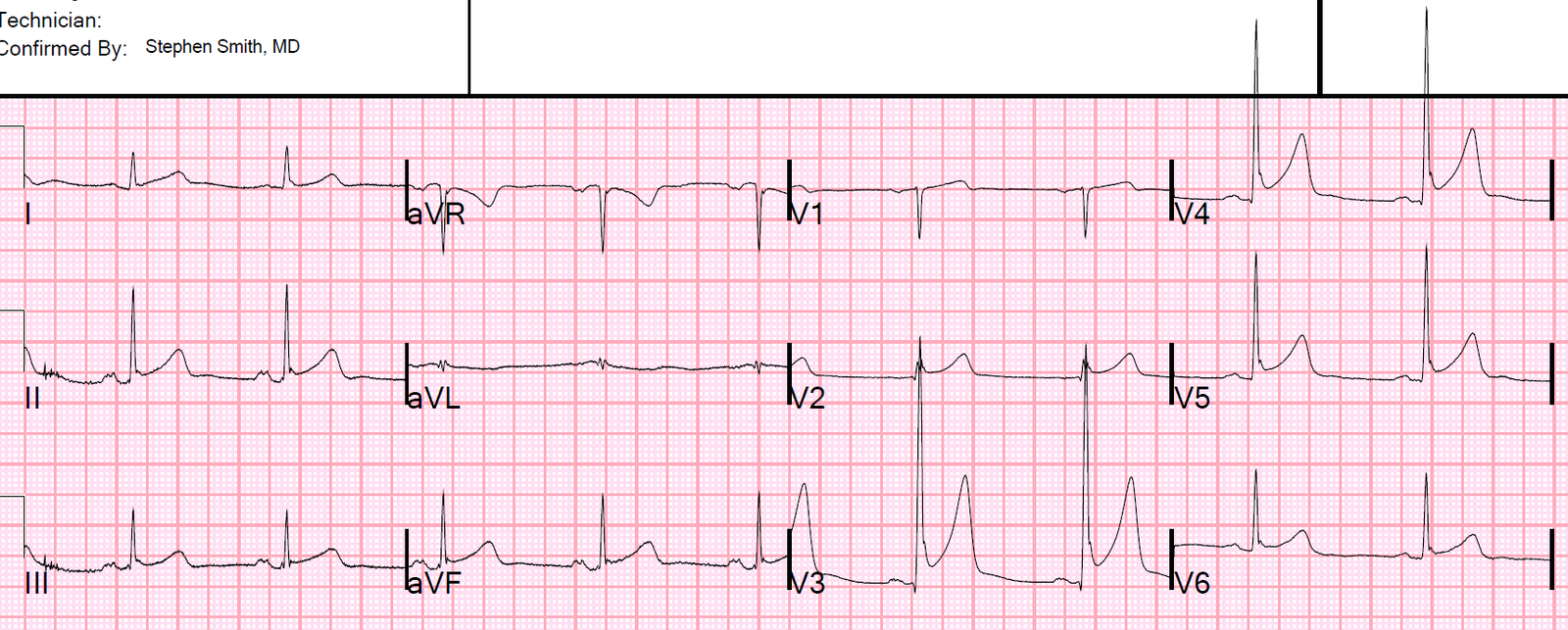
My appreciation to Kenneth Khoo (of Malaysia) for today’s case. This patient was hemodynamically stable. There was debate among providers in his institution as to what the rhythm in this ECG was (Figure-1).
- What do YOU think the rhythm is?
- What is the differential diagnosis?
- Why can you be virtually certain what this rhythm is even before treating and before any diagnostic maneuvers?
= = =
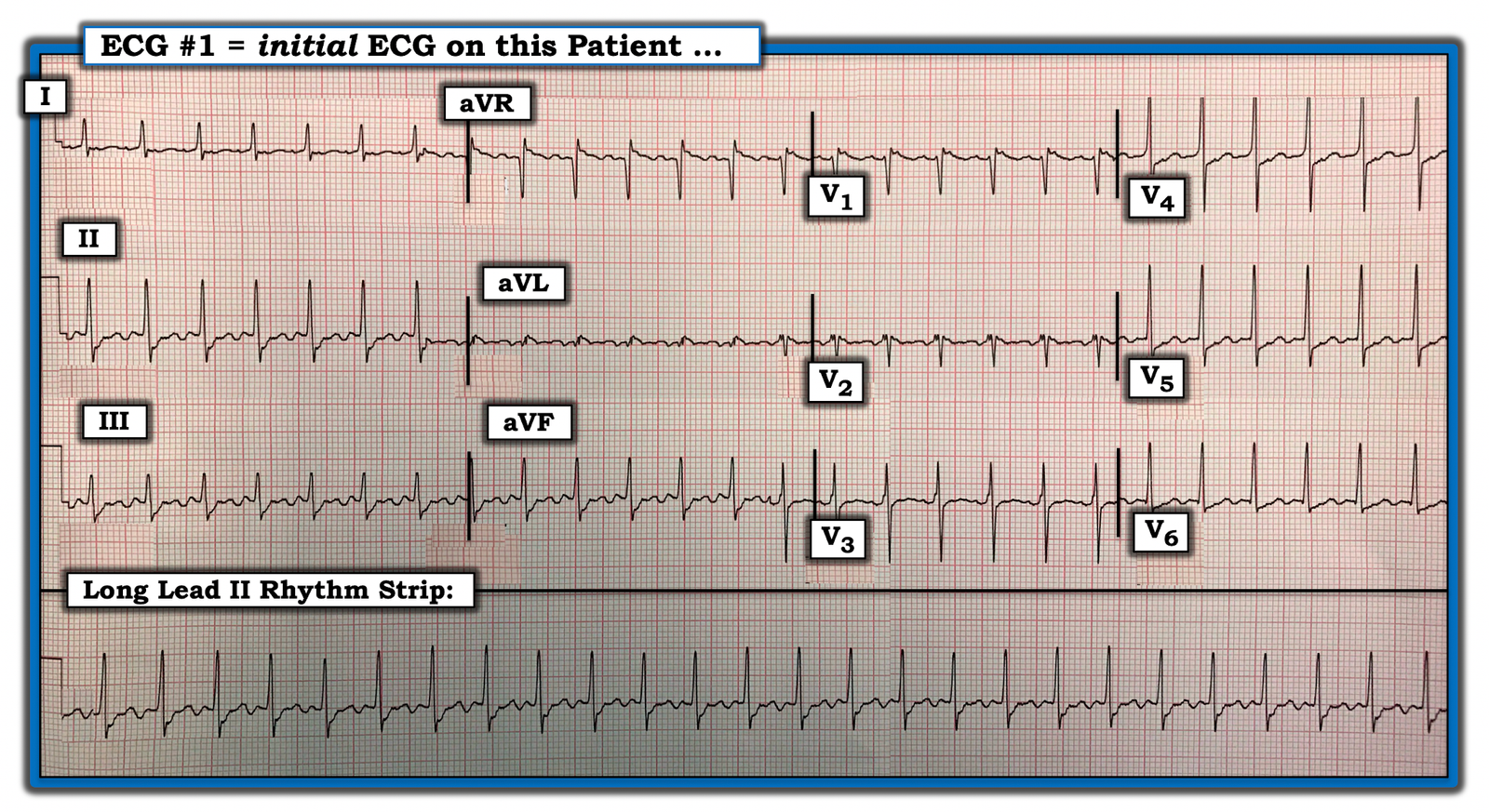
Figure-1: The initial ECG in today’s case.
= = =
My Approach to Today’s Rhythm:
I reviewed the basics for rhythm interpretation in the October 16, 2019 Case from Dr. Smith’s ECG Blog. In brief — once you’ve assured that your patient is hemodynamically stable (as this patient was) — We need to assess the remaining 5 KEY parameters. I favor this memory aid, “Watch your P‘s, Q‘s and the 3 R‘s”:
- NOTE: It does not matter in what sequence you address these 5 KEY parameters — and I often change the sequence I use depending on the tracing (ie, Which of these 5 parameters is easiest to assess in the tracing in front of you?).
- For the tracing in Figure-1 — the rhythm is perfectly Regular. The R-R interval is almost exactly 2 large boxes — which means that the ventricular Rate is 300/2 ~150/minute. The QRS complex is narrow — so this rhythm is supraventricular! Normal atrial activity is not seen — because there are no clear sinus P waves (ie, the P wave is not clearly upright in lead II …).
= = =
QUESTION:
- What does the above analysis suggest to YOU thus far?
= = =
= = =
ANSWER:
We’ve established that this patient is hemodynamically stable. The rhythm in Figure-1 is a regular SVT (SupraVentricular Tachycardia) at ~150/minute without clear sign of sinus P waves. The principal differential diagnosis is similar to what we derived in the October 16, 2019 Case: i) Sinus Tachycardia; ii) Reentry SVT (either AVNRT if the reentry circuit is contained within the normal AV nodal pathway — or AVRT if an accessory pathway is involved); iii) Atrial Tachycardia; — or, iv) Atrial Flutter.
- PEARL #1: The major difference between this case and the case we presented on October 16 — is that the ventricular rate is very close to 150/minute. The most commonly overlooked sustained cardiac arrhythmia (by far) is AFlutter! Over the years — I’ve seen numerous cardiologists overlook this rhythm (especially those cardiologists who do not routinely use calipers for assessment of complex arrhythmias). I fully acknowledge that I’ve overlooked AFlutter.
- The BEST way never to overlook the ECG diagnosis of AFlutter is to: i) Think of this diagnosis often! — and, ii) To assume that any regular SVT rhythm in which clear sinus P waves are not seen is AFlutter until you prove otherwise — especially IF the ventricular rate of this reguar SVT rhythm is close to 150/minute (usually between ~140-160/minute range — but occasionally within ~130-170/minute).
- PEARL #2: The reason the ventricular rate for AFlutter is so often close to 150/minute — is that: i) The atrial rate for untreated AFlutter is almost always close to ~300/minute (ie, 250-350/minute range) — and, ii) Untreated AFlutter most often conducts with a 2:1 ventricular response (ie, atrial rate ~300/minute — therefore ventricular rate ~300/2 = ~150/minute).
- PEARL #3: The expected atrial rate for flutter is likely to change IF the patient has been “treated” — in which case the ventricular rate in AFlutter with 2:1 AV conduction may be slower (if the patient is on antiarrhythmic medication) — or possibly even faster (if he/she has been treated by ablation).
= = =
QUESTION: We said that normal sinus P waves were not seen for the rhythm in Figure-1 — because there is no clearly upright P wave in lead II.
- Does this mean that there is no atrial activity in Figure-1?
= = =
ANSWER: There appear to be lots of “extra deflections” in a number of leads in ECG #1 …
- PEARL #4: The BEST way we know to quickly determine if the “extra deflections” that we seem to be seeing in ECG #1 represent atrial activity — is to use calipers!
= = =
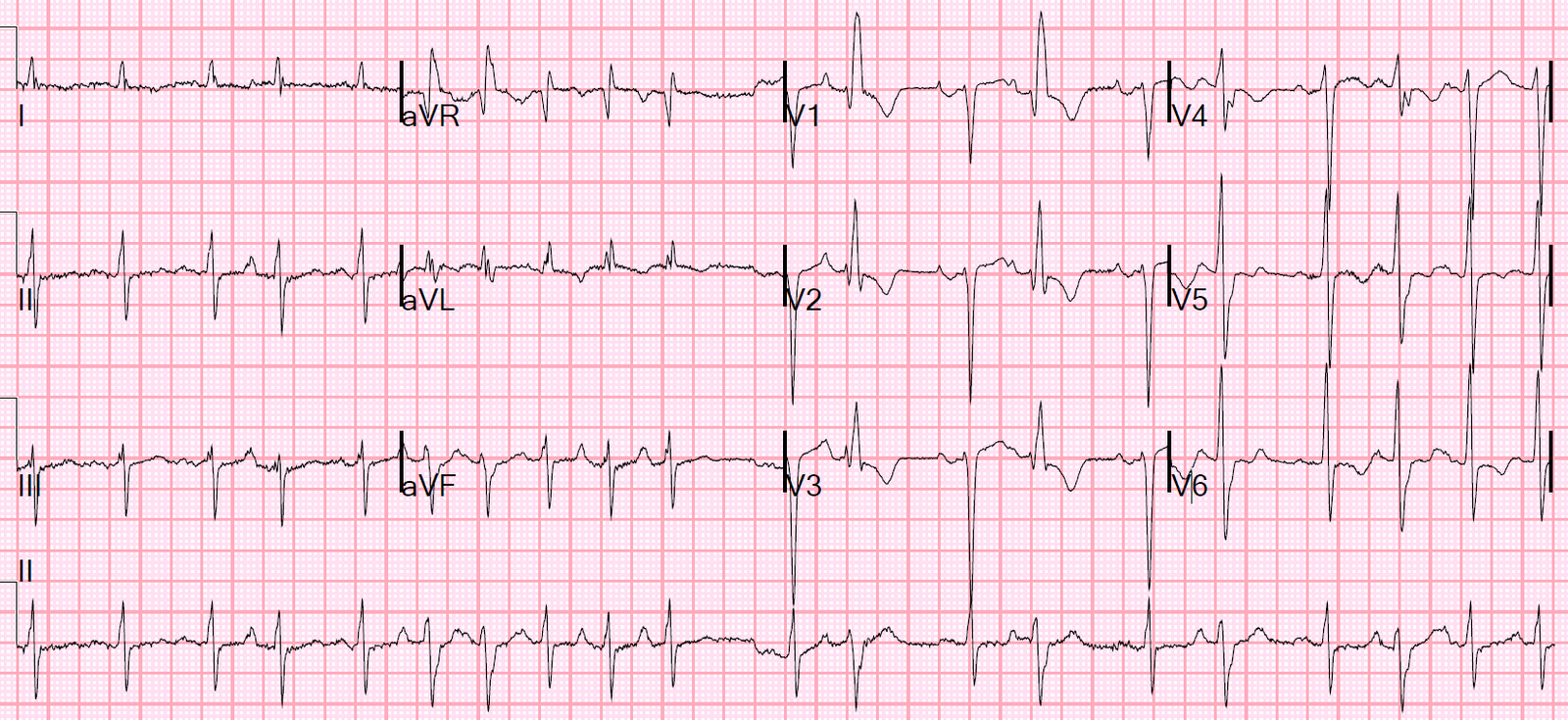
We show the result of using calipers in Figure-2:
= = =
Figure-2: RED arrows indicate that the “extra deflections” are indeed regularly occurring in multiple leads.

= = =
Looking for Flutter Waves: The diagnosis of AFlutter can be established in a regular SVT at ~150/minute — IF you are able to identify regular atrial activity at ~300/minute. Nothing else results in a regular atrial activity at this fast of a rate (Atrial tachycardia will rarely be faster than 250/minute).
- PEARL #5: The way I look for flutter waves is to carefully set my calipers at precisely HALF the R-R interval of the regular SVT (since IF the rhythm is AFlutter — then the atrial rate should be twice the ventricular rate if there is 2:1 AV conduction). RED arrows in Figure-2 confirm that there is indeed 2:1 atrial activity in this tracing — which tells us even before application of a vagal maneuver or administration of Adenosine (or other AV node blocking agent) that the rhythm is virtually certain to be AFlutter.
- PEARL #6: My “GO TO” leads for identifying atrial activity are: i) Lead II — which is typically the BEST lead for identifying atrial activity. In AFlutter — leads III and aVF also usually provide ready evidence of 2:1 atrial activity; ii) Lead V1 — next to lead II, lead V1 is often the 2nd-best lead in my experience for identifying atrial activity. With AFlutter — one will often see positive deflections similar to those seen in Figure-1 in this V1 lead; iii) Lead aVR is often surprisingly helpful for identifying atrial activity (RED arrows in ECG #1); and, iv) IF none of the above leads suggest atrial activity — then I’ll survey the remaining 7 leads as I look for atrial activity. That said, AFlutter will almost always provide ready evidence of atrial activity in one or more of my “Go To” leads.
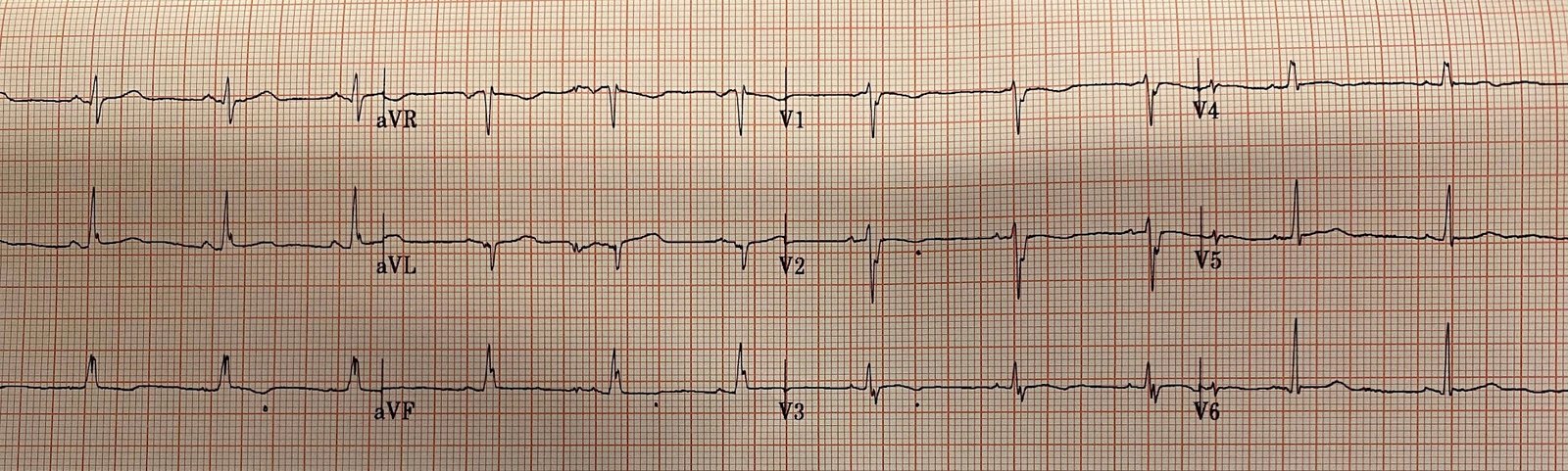
- PEARL #7: On occasion — atrial activity may not be readily apparent in a hemodynamically stable patient with a tachyarrhythmia. In such cases — use of an alternative lead system, such as a Lewis Lead may enhance atrial activity and facilitate rhythm determination. Figure-3 reviews how to use a Lewis Lead. The March 20, 2018 post on Dr. Smith’s ECG Blog illustrates application of a Lewis Lead in a patient in a regular SVT rhythm.
= = =
Figure-3: Use of a Lewis Lead.

= = =
= = =
= = =