A middle aged male presented with chest pain. EMS was called and an ECG was recorded which is virtually identical to the first ED ECG.
The cath lab was activated by the medics.
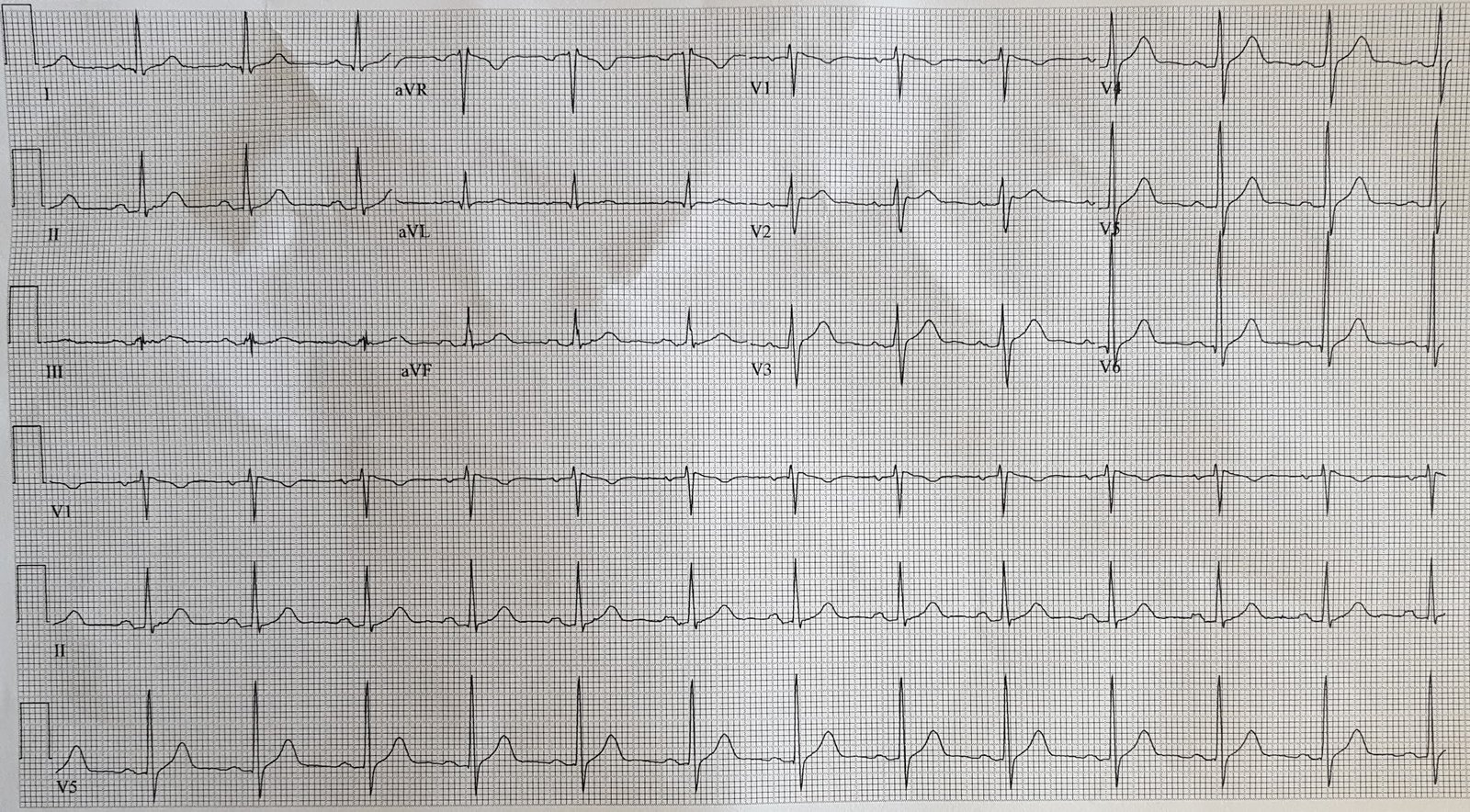
Here is that first ED ECG:
 |
| There is obvious inferior ST elevation, with reciprocal ST Depression in aVL (inferior STEMI).
There is also ST Depression in lead I. This is good evidence that the inferior STEMI is caused by an RCA occlusion. There is ST depression maximal in lead V2. Thus, there is a posterior STEMI. There is also ST depression in V5 and V6. |
Where else is there evidence of STEMI?? (see below)?
There is absence of ST depression in lead V1. Given the profound ST depression (of posterior MI) in lead V2, there should also be ST depression in lead V1, but there is not. This suggests that something is “pulling up” the ST segment in lead V1. In other words, there is relative ST elevation in lead V1. As V1 sits directly over the right ventricle (RV), this suggests STEMI of the RV, which is caused by a proximal RCA occlusion, proximal to the RV marginal branch.
This patient did not have any of the hemodynamic characteristics of RVMI (hypotension, nitroglycerine sensitivity).
However, when I saw this I suspected RV MI and suggested to the treating physician that a right-sided ECG be recorded.
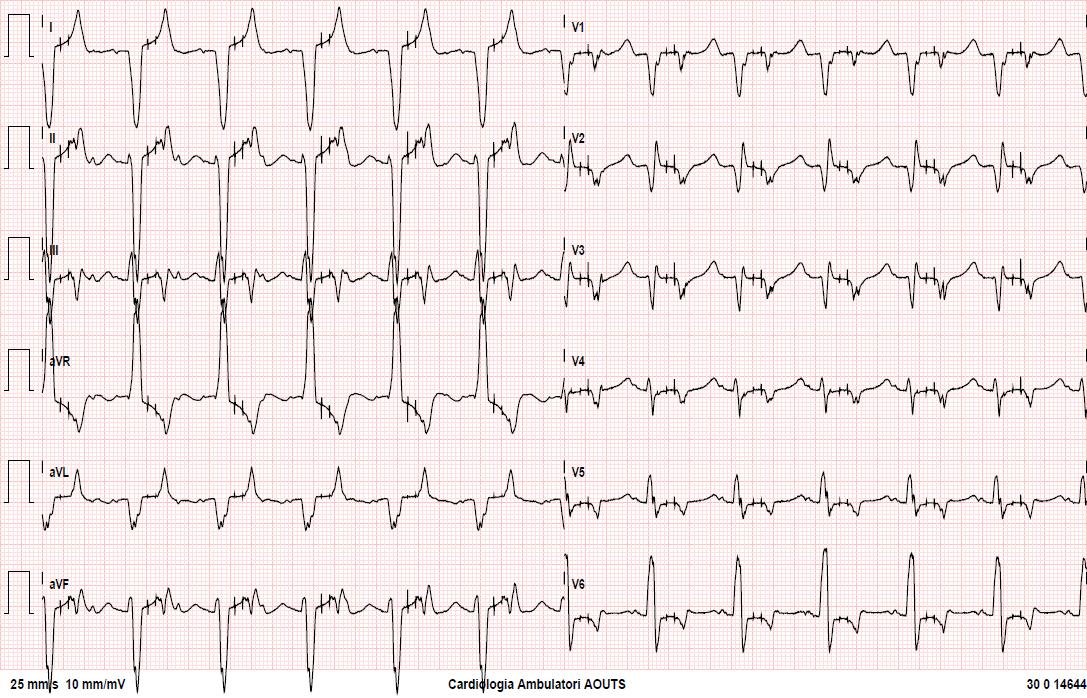
Here it is:
 |
| V1 should be labelled V1R, which is the same lead as V2 V2 should be labelled V2R, which is the same lead as V1 V3 is V3R V4 is V4R V5 is V5R V6 is V6R There is huge ST elevation across the right sided leads, diagnostic of RV STEMI. |
Does this matter? Won’t the interventionalist just find the lesion and fix it?
Furthermore, it is good to know that the RV is involved in order to anticipate right sided heart failure with hypotension and nitroglycerine sensitivity.
How sensitive and specific is STE in V1 in the setting of RV MI, in cases with and without concomitant ST depression in lead V2?
We are just finishing a manuscript on this and cannot reveal our results. Suffice it to say that STE in V1 is pretty specific but not sensitive. Furthermore, that ST depression in lead I, though it does predict RCA occlusion, does not give any further information about whether that RCA occlusion is proximal (RVMI) or not.
In other words, all patients with inferior STEMI should have a right sided ECG recorded.