An 83 yo complained of palpitations and dizziness and presyncope. He had a history of systolic heart failure with an EF of 40-45% and h/o coronary stents. He is on digoxin and coumadin for atrial fib. He denied chest pain or shortness of breath. EMS arrived and noted HR in the 170’s. He was not in shock. There was no pulmonary edema. Mental status and blood pressure were normal.
They recorded the following rhythm strips:
V5
 |
| A very wide complex regular tachycardia. By ECG alone (without considering pretest probability), the differential is VT vs. SVT with aberrancy vs. AVRT vs. very fast sinus with aberrancy. The QRS width and the time from onsent of R-wave to nadir of S-wave is typical of VT (greater than 100 ms). |
Here is lead II
 |
| This does not add much to the above. |
This is a regular wide complex tachycardia. I see no P-waves, antegrade, retrograde, or dissociated. The QRS is very wide.
They attempted adenosine, first 6 mg, then 12 mg, with no change.
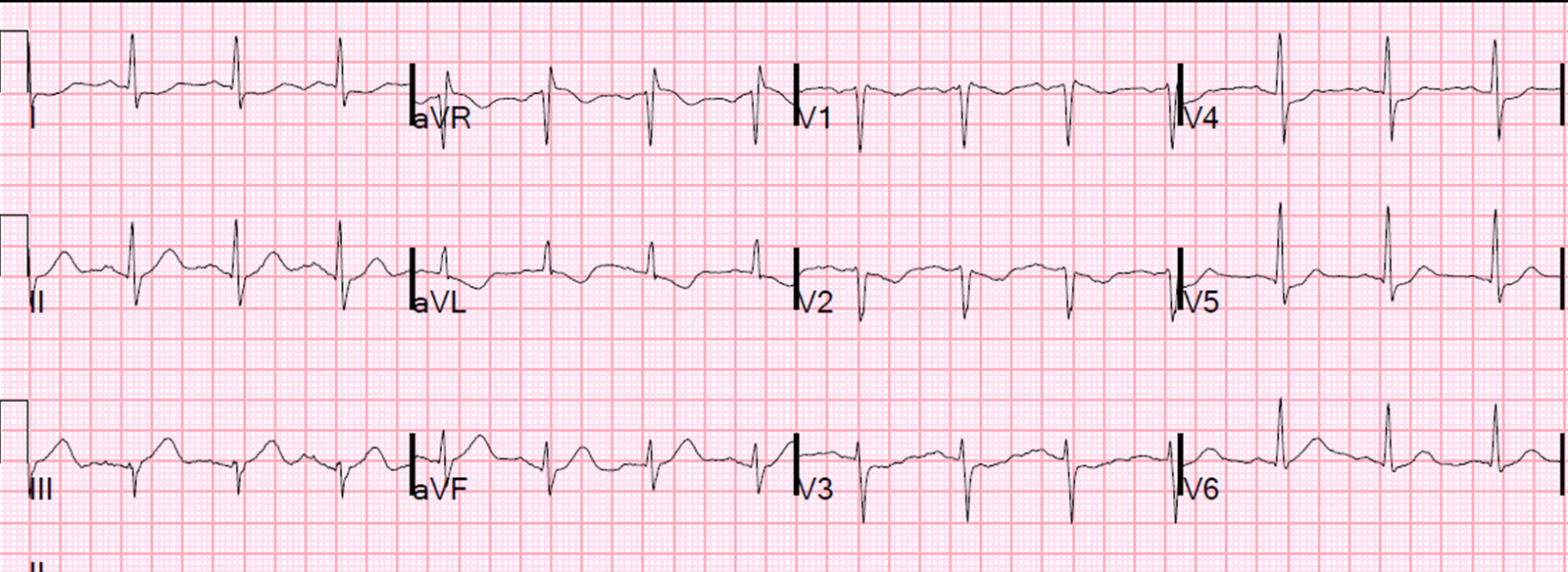
On arrival, the patient was very stable. In the ED, this 12-lead ECG was recorded:
 |
| What is the diagnosis? |
The diagnosis is VT, for many reasons. For those who can perform procedural sedation safely, the appropriate therapy is sedation with electrical cardioversion. In such a stable patient, if sedation cannot be performed safely, an antidysrhythmic such as ajmaline, procainamide, or sotalol (or lidocaine) may work. None are as dependable as electricity.
See annotated ECG:
 |
|
–Black lines show the onset of the QRS in all 12 leads, as determined from finding the onset of the QRS in lead I –Green arrows. Using the black lines to find the onset, these arrows then illustrate the onset and end of the QRS in V1, such that one can determine the QRS duration is about 200 ms. This is too long for SVT with aberrancy –Blue arrow shows the wide q (lower case)-wave, which indicates prolonged duration of initial depolarization, also consistent with VT –Red circle shows the right bundle morphology with RR’ (first R has greater voltage, unlike true RBBB), also consistent with VT –Black arrow shows the nadir of the S-wave in V6: from onset of R-wave to nadir of S-wave is at least 100 ms, also consistent with VT. |
When determining VT vs. SVT, here is the sequence of analysis I use:
Consider in the context of clinical scenario.
(None of this applies to fascicular VT or RV outflow VT, which are associated with normal heart structure and originate in or near conducting fibers. However, these are rare exceptions):
a. VT is more common than SVT among WCT
b. Older patients are more likely still to have VT
c. Any history of cardiomyopathy, MI, structural heart disease, or coronary disease makes VT much more likely
And then consider the ECG.
The unifying principle of most VT is that the first part of the QRS is initiated in myocardium, NOT in conducting fibers, and thus conducts slowly. Therefore, the initial part of the QRS changes its voltage SLOWLY (wide). This is what I look for to diagnose VT:
1. The longer the QRS, the more likely it is VT. A QRS duration greater than 140 ms is likely VT, though it is not a terribly reliable differentiator. However, a QRS duration of 200 ms is almost always VT or aberrancy with hyperkalemia. This case is thus almost certainly VT.
2. Obvious AV dissociation? Then VT, if not:
3. Obvious fusion beats? If so, the VT, if not:
4. Leads V1-V6 unidirectional (no RS or SR) and “concordant“ (in the same direction)? Then VT
5. If there are RS complexes (they are not concordant): is there any precordial RS that has a duration from onset of R to nadir of S that is greater than 100 ms? Then VT.
6. Abnormal LBBB or RBBB pattern (see this link for a figure from the Brugada paper):
—-a normal RBBB or LBBB pattern makes SVT very likely: both have a rapid initial deflection, the r-wave in LBBB and the rS in RBBB, followed by a slowly conducting latter part of the QRS.
a. If there is LBBB pattern, is the initial r-wave greater than 50 ms? Or is the onset of the QRS to nadir of the S-wave in V1-V3 greater than 60-70 ms? If so, this is not true LBBB. VT.
b. If there is RBBB pattern, is there a monophasic R-wave? Or is the first R of the Rsr’ larger than the second one? Then VT.
7. Initial R-wave in aVR (not an r-wave, not preceded by q-wave)? Then VT
8. If the initial deflection in aVR is an r-wave or q-wave, is it greater than 40 ms? If so, then VT
In this case, the physicians were confused by the ECG. (With some practice, this ECG should not be confusing!)
They placed Lewis leads (see below for instructions). See this link for graphic instructions on how to use Lewis leads; it is very easy. Why? Lewis leads are good for illuminating P-waves. The physicians wanted to see if there were P-waves, and, if so, whether they were associated or dissociated. AV dissociation with normal upright P-waves is nearly diagnostic of VT (not 100%), and regular upright P-waves followed consistently by QRS complexes would be nearly diagnostic of sinus tachycardia with aberrancy. On the other hand, retrograde P-waves would not necessarily differentiate SVT with aberrancy from VT.
Rhythm strip with Lewis leads:
 |
| There is an axis change that is due to the lead change. Lead I is the most important lead and it is highlighted below: |
Lead I is the important lead in Lewis leads. Here is lead I alone:
 |
| The Lewis leads appear to have made the P-waves in lead I more visible. They are inverted, and start after the beginning of the QRS. They are associated with each QRS.
This would rule out sinus as the rhythm, but it still does not differentiate between 1) SVT with aberrancy and retrograde P-waves and 2) VT with retrograde P-waves. |
They saw these P-waves, but did not understand that they could also be the result of VT.
So they gave adenosine 18 mg. It did nothing. Adenosine is perfectly safe in VT. However, it will have no effect.
At this point, they appropriately sedated the patient and electrically cardioverted.
The post conversion ECG is here:
 |
| Atrial fibrillation with some mild ST depression. There are inferior Q-waves. |
Clinical Course:
ECG and Transthoracic Echo confirmed prior inferior infarction. Angiogram confirmed known severe RCA disease. There was no new ischemia.
Thus, this was scar-mediated VT. An ICD was placed.
Learning points:
1. Sometimes it is difficult to differentiate VT from SVT with aberrancy. In this case, the diagnosis should be clear. There are multiple variables to look for and many were present here, especially the pretest probability of VT.
2. Adenosine is safe in VT. However, you could convert adenosine sensitive RV outflow tract VT and not realize it. However, these have no structural disease and are safe.
3. Lewis leads help to see P-waves. Associated retrograde P-waves can be present in VT as well as SVT.