Disclaimer: I never state from where I get a case. They come from all over the world. Any case may or may not be from my own institution. Do not make any assumptions.
Case:
A non-English speaking woman in her 60’s with h/o HTN, type II DM, hyperlipidemia, CAD s/p CABG 16 years prior, and end stage renal disease on dialysis presented to the ED at time 0. She had awoken 7 hours prior with severe headache followed by upper chest heaviness and vomited x 2. EMS placed an 18 gauge IV, gave 2 NTG, and aspirin. She stated the pain was not similar to a previous MI. BP was 200 systolic. The patient stated that her chest pain was more of an issue than her headache.
Here is her initial ECG:
 |
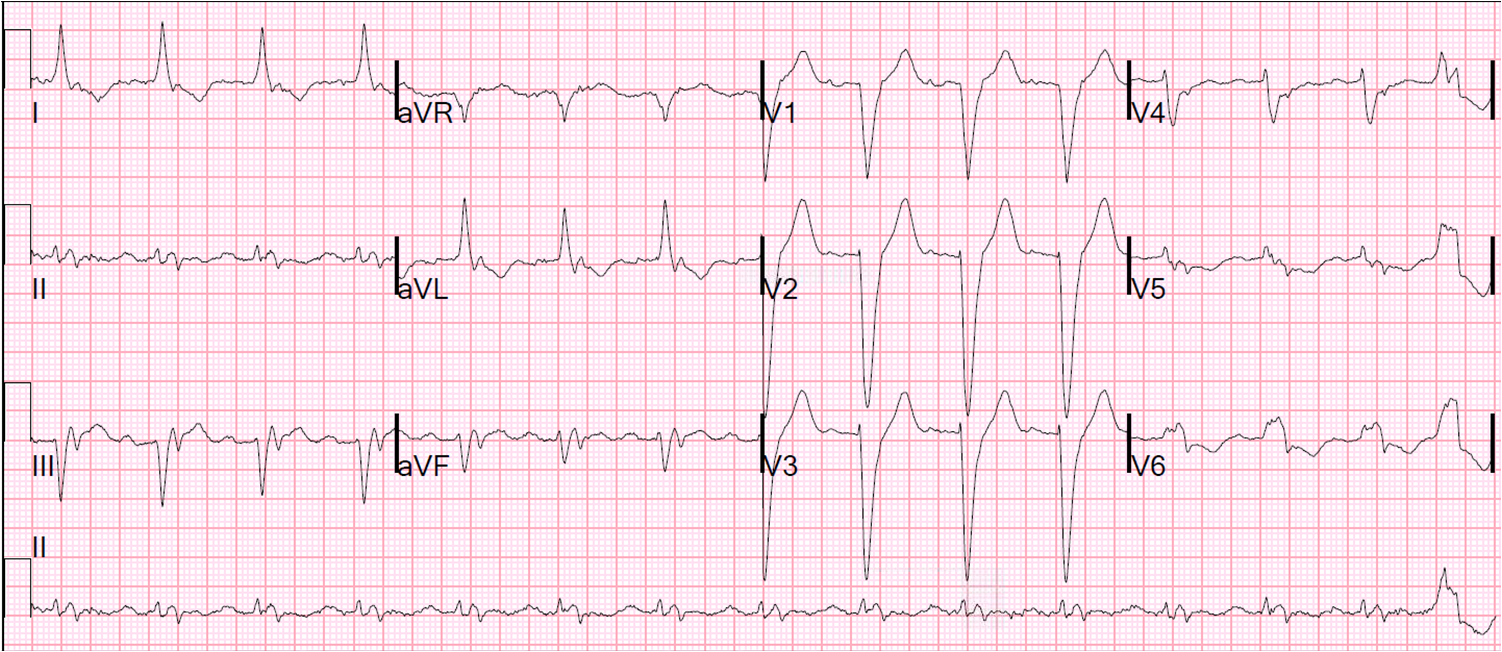
| There is sinus rhythm, left axis deviation (probable LAFB), and new ST elevation in V1-V3. What do you think? See more discussion below. |
What was not seen is that there is QRS widening (120 ms) and peaked T-waves diagnostic of hyperkalemia and a pathognomonic, though unusual, pseudoSTEMI pattern. Cardiology was called and the cardiologist activated the cath lab.
The angiogram showed no acute disease. However, following the procedure, during the sheath pull, she
experienced VT arrest and was administered multiple shocks for wide complex tachycardia. 3 “amps” of lidocaine, 300 mg amiodarone, Sodium Bicarbonate x 2 “amps”, D50 x 1 “amp”,
and calcium gluconate x 1 “amp” were all given. She had return to sinus rhythm with narrow complex. After resuscitation, she was comatose and was intubated.
It is uncertain when the K returned, but it was 7.5 mEq/L when it did.
Here is the post-resus ECG:
 |
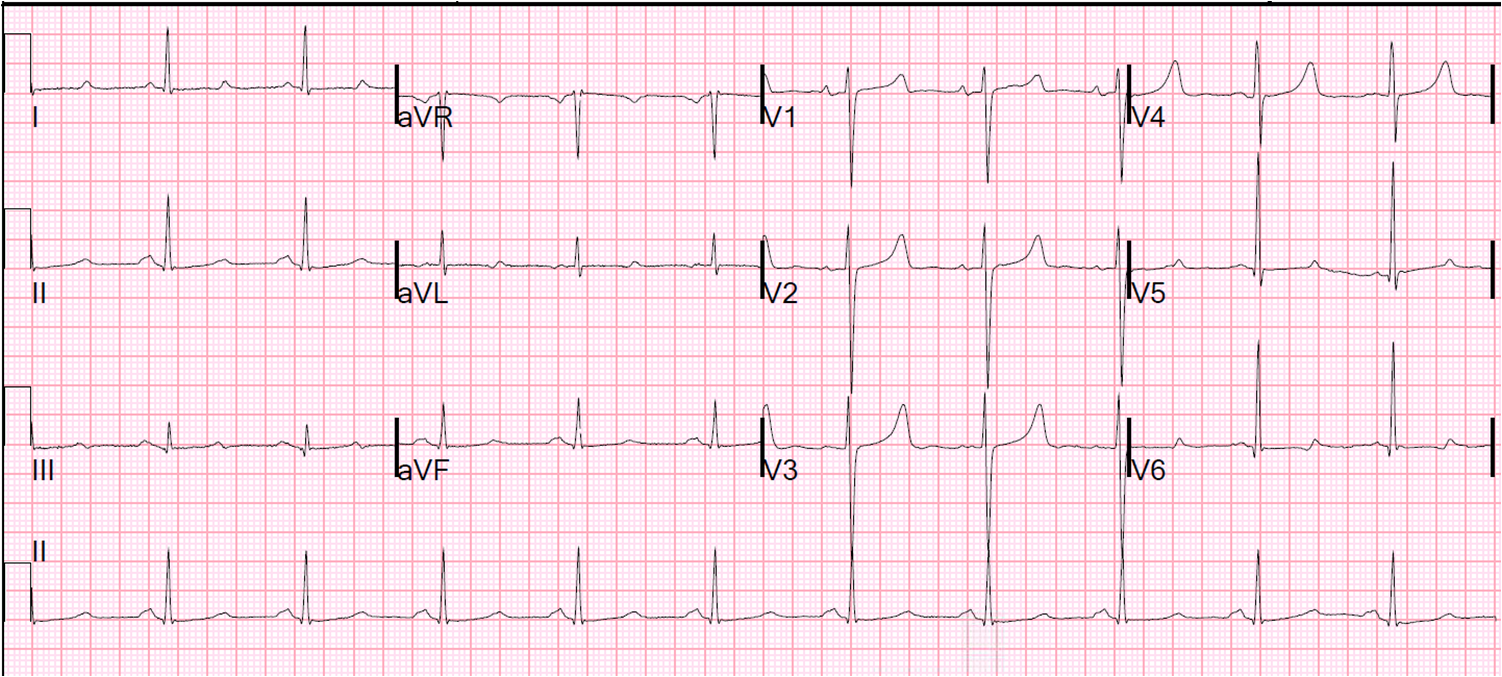
| Now there is sinus bradycardia with an accelerated junctional rhythm and AV dissociation (no evidence of AV block on this ECG). There is diffuse T-wave inversion, with massive T-waves, all but diagnostic of stress cardiomyopathy. |
The stress cardiomyopathy gets even more pronounced here (20 minutes after the previous):
 |
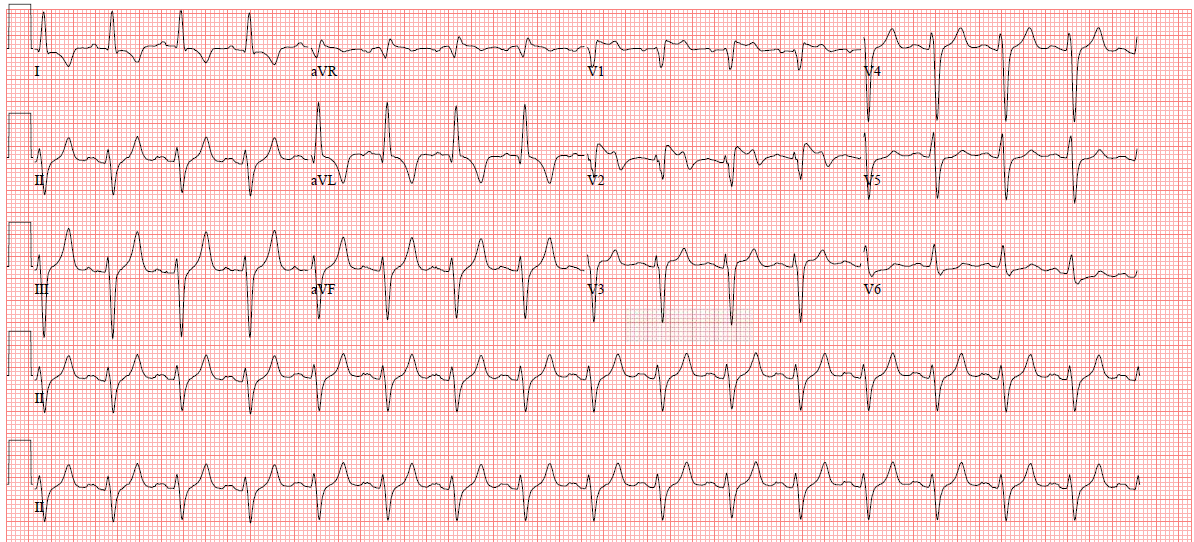
| Sinus brady with nodal escape and AV dissociation persists. T-waves are massive and bizarre, with precordial T-waves inverted. |
Echo confirmed tako-tsubo like apical ballooning of stress cardiomyopathy. The stress was doubtless her cardiac arrest.
She was dialyzed, cooled (therapeutic hypothermia for comatose survivor of cardiac arrest). One of my blog followers (an EM G2) was on the neurology service and recognized the initial ECG pattern as diagnostic of hyperkalemia. He could do so because of these previous posts (and because he is very smart, hard-working, and attentive):
Hyperkalemia PseudoSTEMIs
Patient course
The patient awoke and went to rehab. She was discharged with some minor neurologic deficits.
Lessons:
1. Remember this pattern of ST elevation in hyperkalemia. It is an unusual but pathognomonic pseudoSTEMI pattern
2. Potassium will hurt you and your patients if you are not always thinking about it!