Here are two different series of ECGs in 2 different patients with chest tightness/discomfort that resolved.
Case 1
A 20-something with chest tightness that later resolved. Blood pressure was normal.
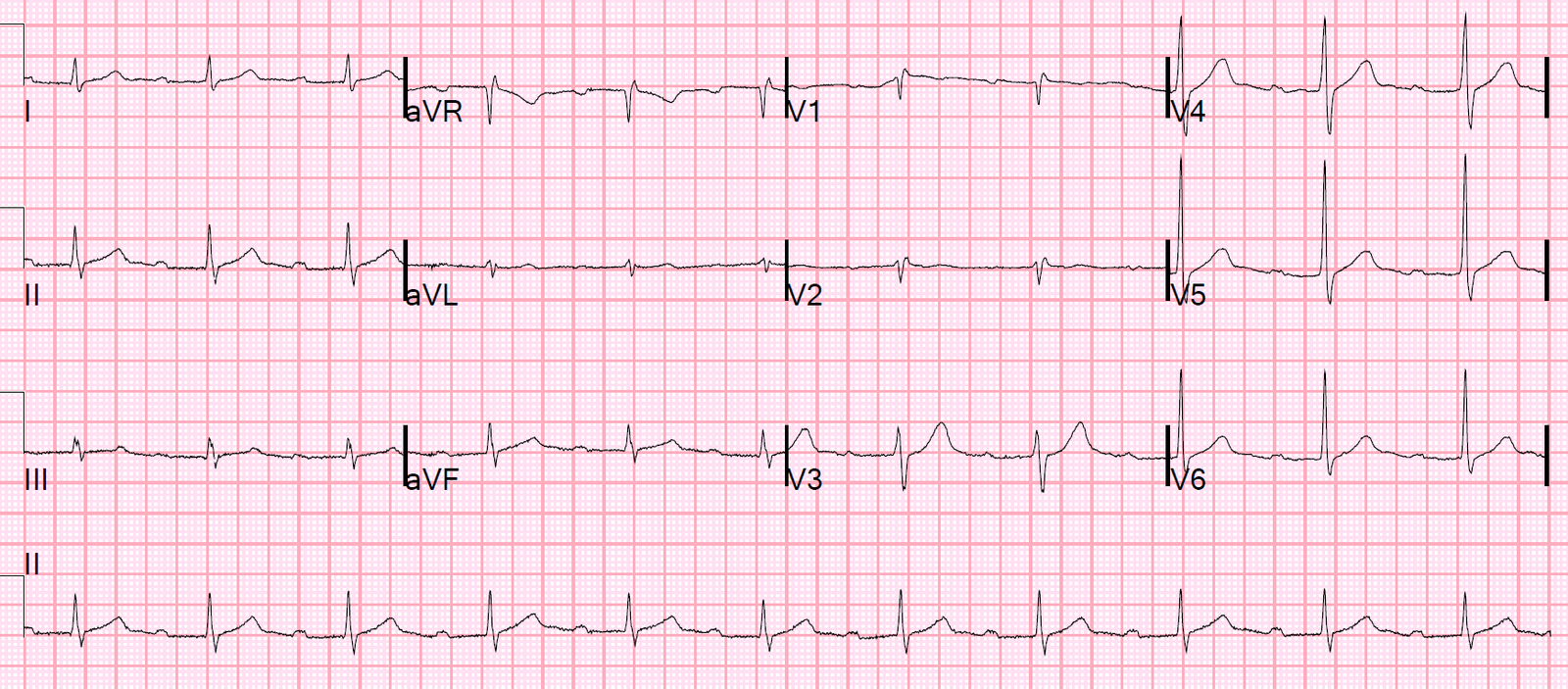
ECG, with chest tightness:
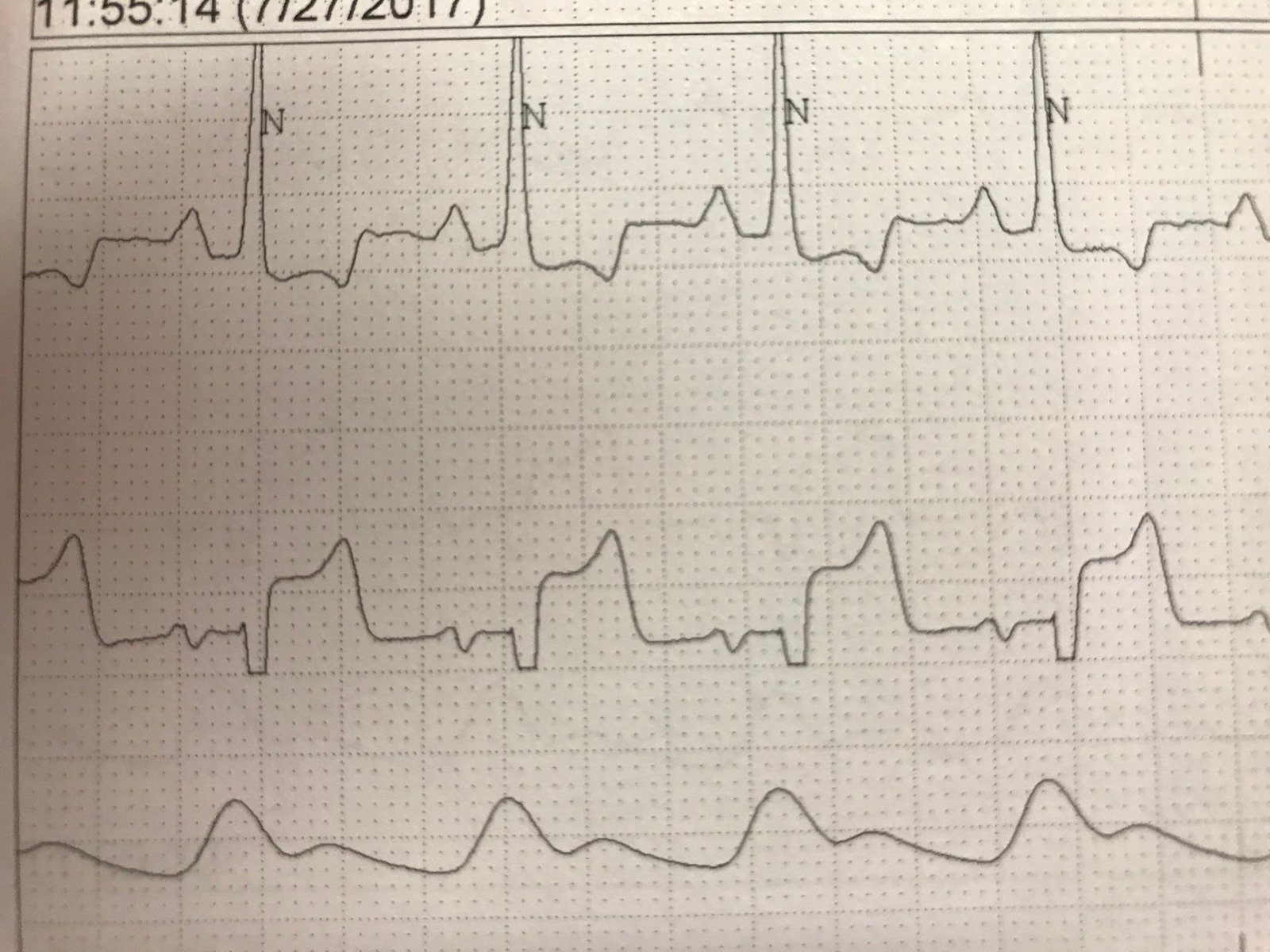
Later ECG, after resolution of chest discomfort

Later, continued pain free

What is your impression?
Case 2
A 50-something with substernal chest pressure all night, now resolved.
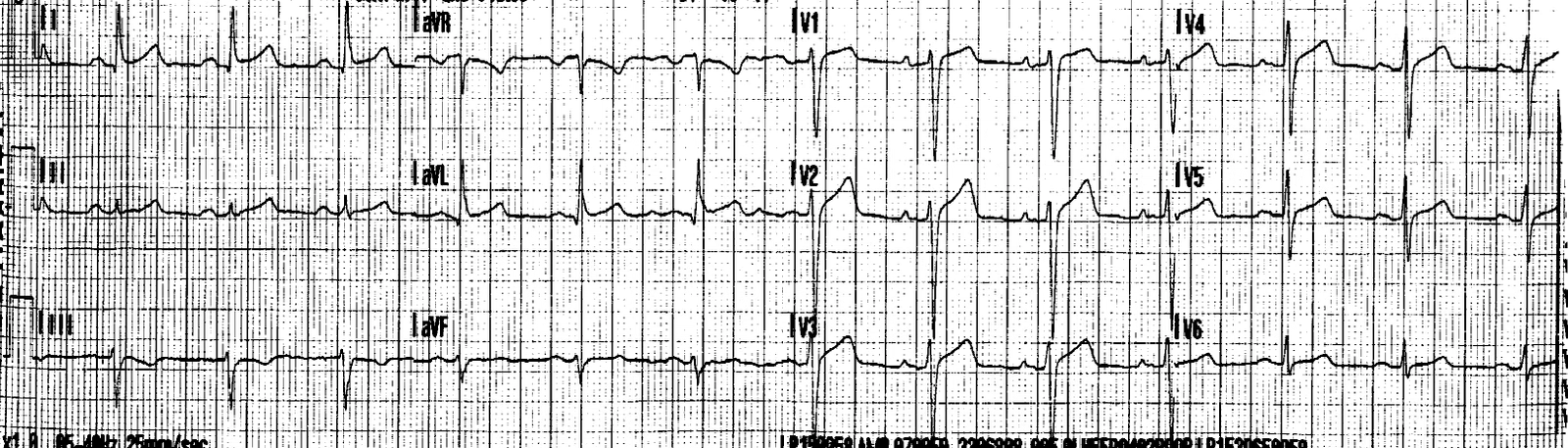
Time zero, pain free

25 minutes, still pain free

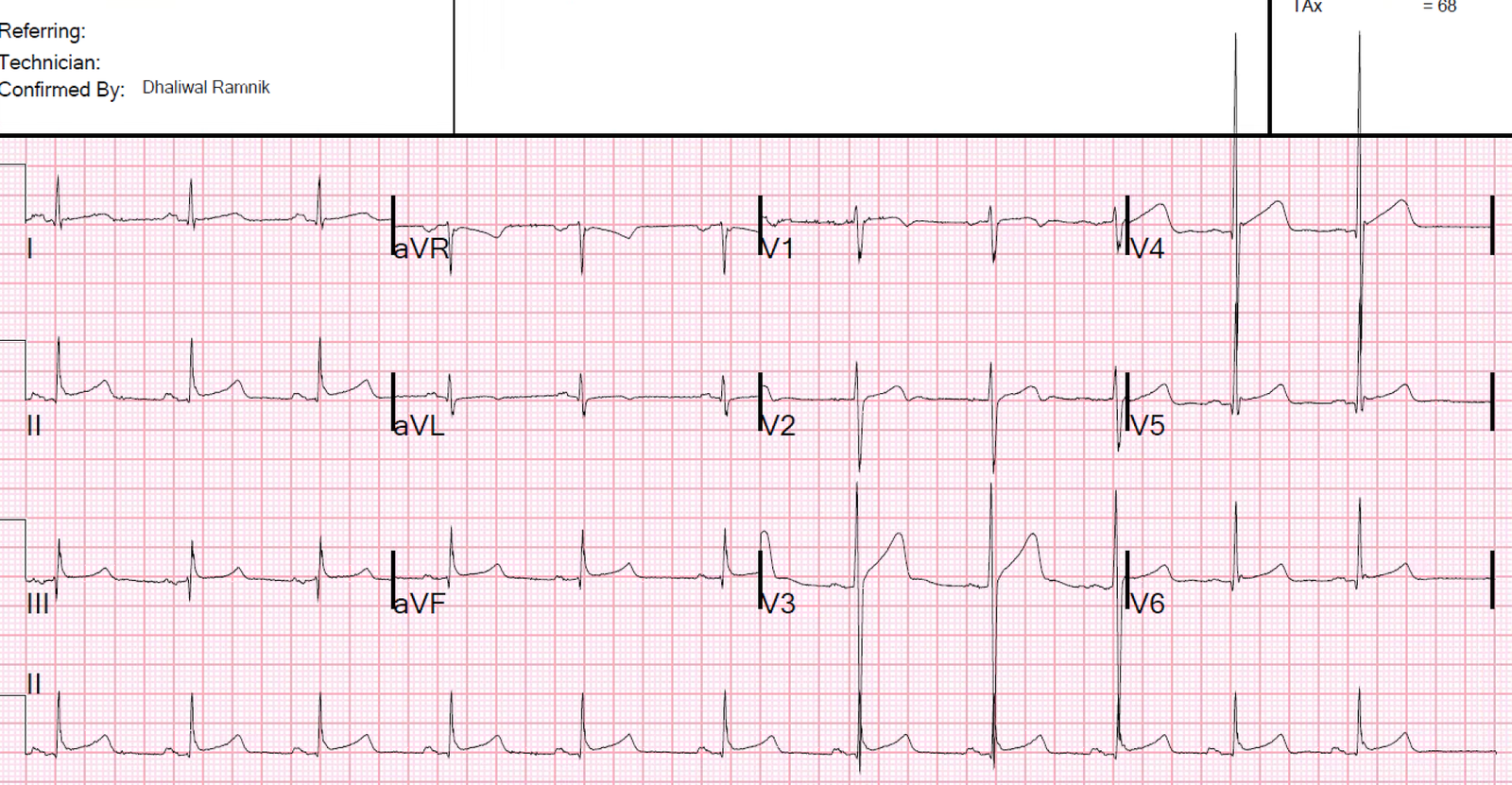
6 hours

Next AM

What is your impression?
Here are ECGs side by side for comparison:
 |
|
Case 2 is on the left Case 1 on the right
–Note on the left (Case 2) there is normal QRS voltage, whereas the voltage on the right (Case 1) is very high. –Notice that on the right (Case 1), V4, along with having high voltage, has a small S-wave and a prominent J-wave. –On the right (Case 1), in V2 and V3, notice the large U-wave. –V2 on the left (Case 2) is somewhat of an anomaly, with a qR-wave suggesting incomplete RBBB; try to ignore it for the purposes of this discussion. These are all features of normal variant T-wave inversion. |
Case 1:
This is classic for a benign pattern, especially in a young athlete. You might be surprised that benign patterns can be dynamic (change with time), but they can be!!
Also telling is that when the patient had pain, he did not have a STEMI pattern. Since Wellens’ syndrome is the pain-free aftermath of an episode of chest pain associated with LAD occlusion, then at the time of active pain at which time an ECG was recorded, the ECG should have shown some evidence of STEMI, or at least of subtle acute LAD occlusion. This first ECG is a normal variant ST elevation in a young male, with high voltage. It does not represent LAD occlusion.
In such a case, one should not assume a benign etiology, but use serial troponins to verify that you are correct. While it is true that, on rare occasion, Wellens’ syndrome may have negative serial troponins, all such cases that I have seen were with earlier generation (less sensitive) troponins.
Outcome:
All troponins were below the level of detection up to 16 hours after presentation.
Case 2:
These ECGs are classic Wellens’ pattern, but also with an unusual lead V2. I saw this patient and immediately knew the diagnosis. The initial troponin I was 1.2 ng/mL (99% URL is 0.030 ng/mL).
He went very quickly to the cath lab and had an 80% thrombotic occlusion of the LAD with TIMI II flow.
The “6 hour” and “Next AM” ECGs are after stent placement.
Learning Points:
1. Not all dynamic terminal T-wave inversion after resolution of chest pain is Wellens’ syndrome.
2. Normal Variants may evolve.
3. There are features of normal variants that distinguish them from Wellens’ waves.
4. Pretest probability is also important: 20-something vs. 50-something with chest pain. That said, young people do get atherosclerotic plaque rupture and MI, and are easily dismissed! See this case:
An intoxicated, agitated, 20-something with chest pain
Other Relevant Posts
Click on this link for a more complete discussion of T-wave inversion normal variants.
This case is amazing: Chest pain, Dynamic ST Elevation and T-waves, and High Voltage
So is this case: Is it important to recognize LVH Pseudo-infarction patterns?
Click here for more PseudoWellens cases.