
This 18 year old presented with syncope and tachycardia.
 |
| Similar to the last case (the “quiz”), there is sinus tachycardia with precordial T-wave inversion with TW inversion in lead III also. The morphology of these T inversions is highly suggestive, but unlike the previous case, not diagnostic. There is also, arguably, S1Q3T3 depending on whether one considers the S-wave to be “prominent.” There is no right axis deviation, but there is a S-wave. (Does anyone know of a definition of “prominent” S-wave in S1Q3T3?) |
Immediately, a bedside echo was done. Here is the video:
This shows a huge and poorly functional RV.
Here is a still picture from the video:
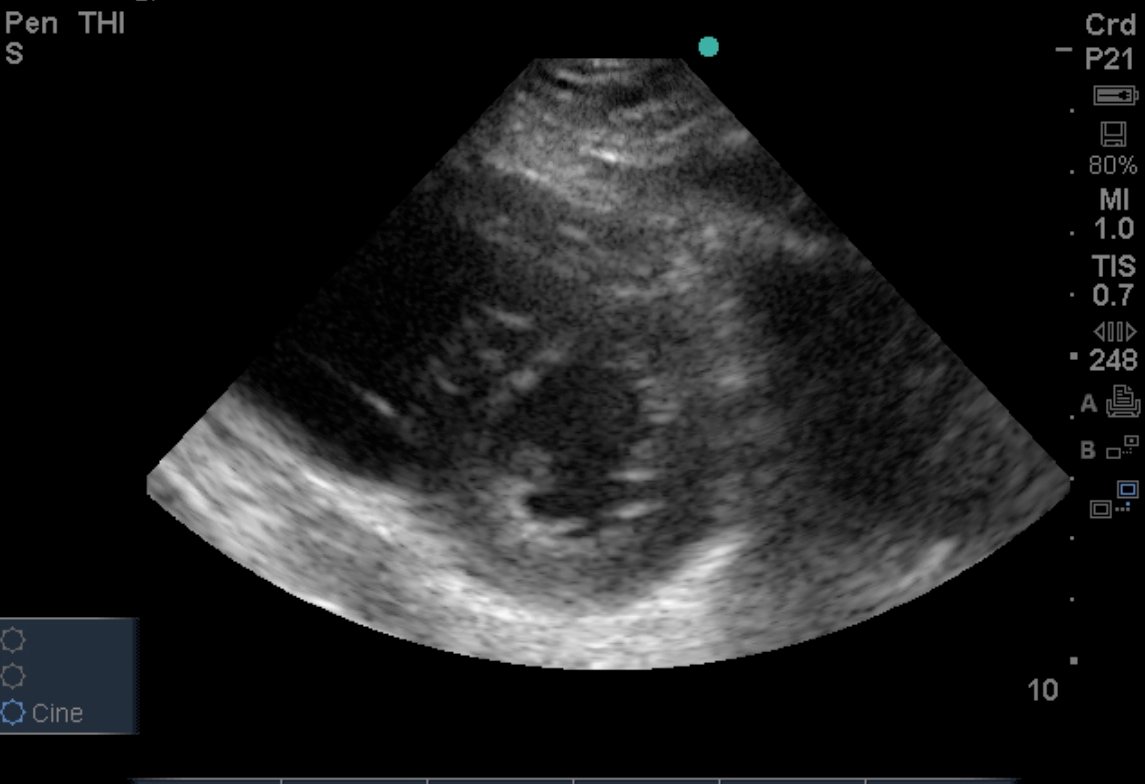 |
| The RV is on the left, the LV on the right (thick-walled). The RV is very enlarged and looks like a “D”. Accordingly, this is called the “D” sign. |
This is diagnostic for pulmonary embolism, which was subsequently proven. Thrombolytic therapy might have been given, but at least partly because of head trauma from syncope, it was not.

