
This 61 year old has a h/o CABG 20 years prior. Onset of chest pain 1 hour prior to calling 911. Here is the prehospital ECG:
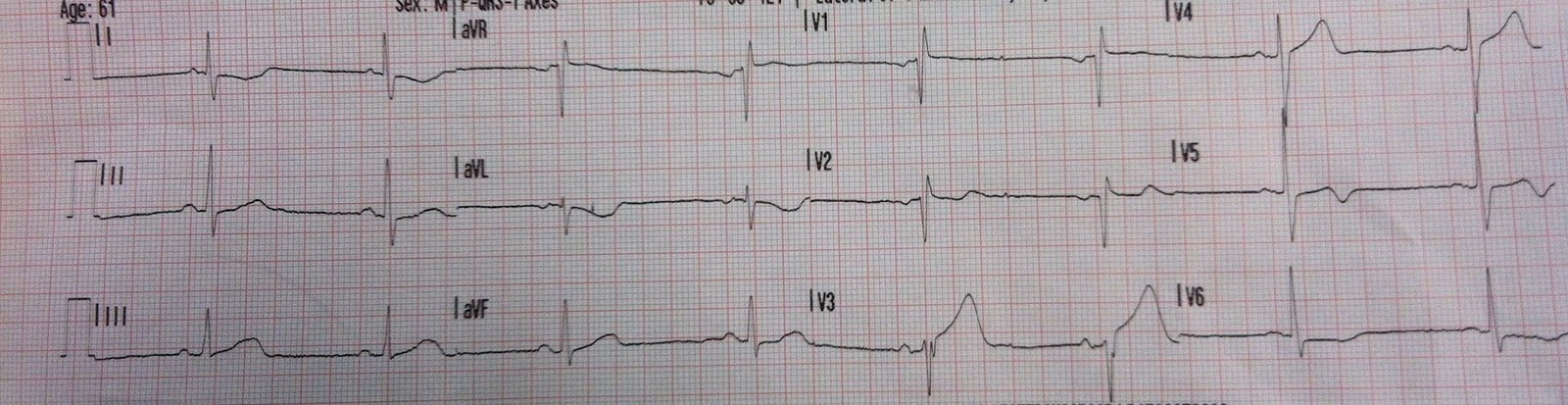 |
| Sinus rhythm. There is an inverted T-wave in I and aVL, with very minimal ST depression, but no inferior ST elevation. The T-wave in III does not have the normal amount of upward concavity. There is a minmal right ventricular conduction delay (R’ in V1). There is a biphasic T-wave in V2, and a quite large T-wave in V3 as well as inversion in V5 |
The only finding that is highly suspicious for ACS in this tracing is the ST segment and T-wave in aVL. These two findings are early findings in inferior STEMI.
He arrived in the ED and had this ECG:
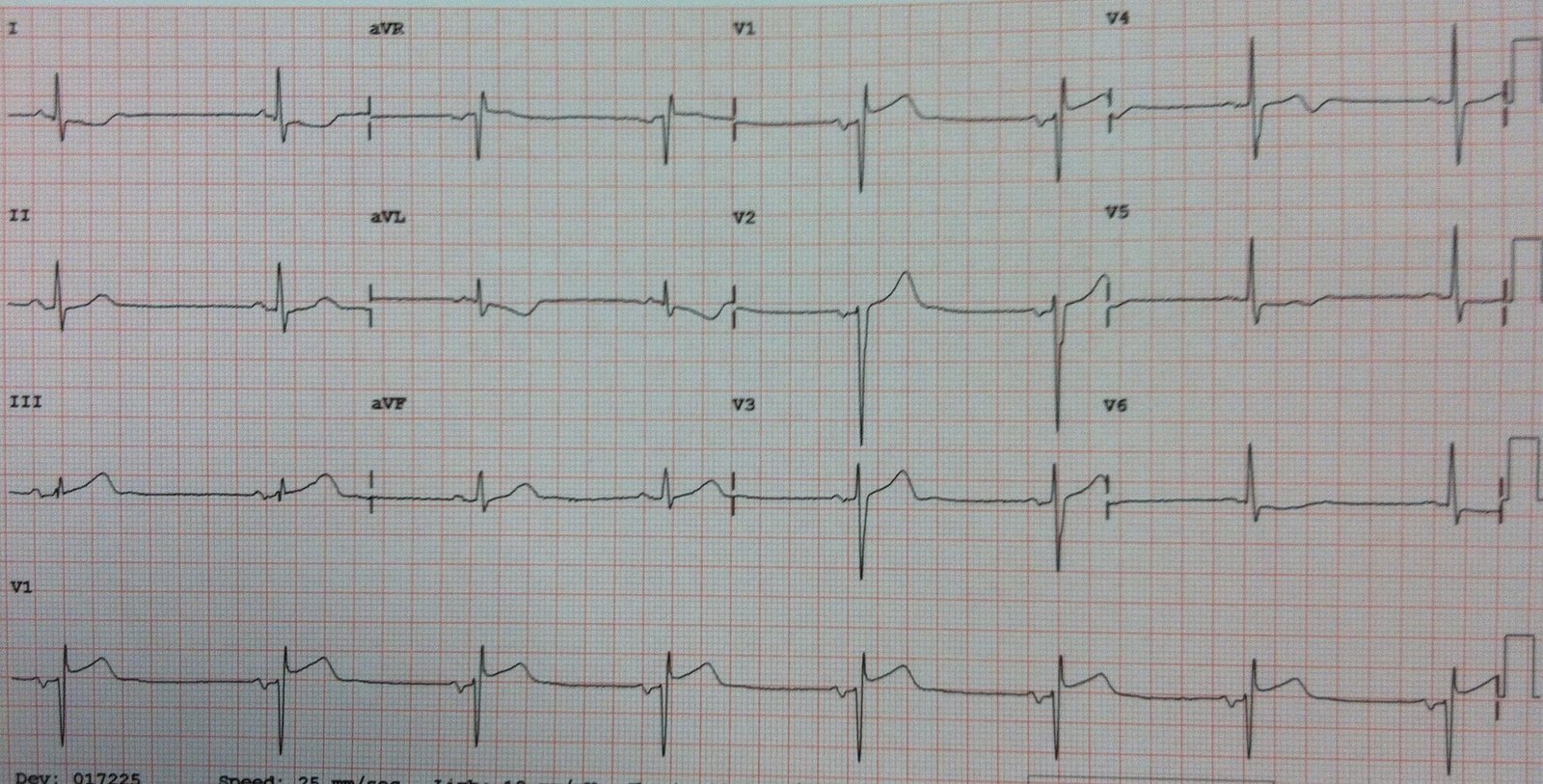 |
| Now the findings in aVL are more pronounced, and the T-wave in lead III looks hyperacute, but still without ST elevation. Also, there is ST elevation in V1, a common sign of right ventricular STEMI |
A right sided ECG was obtained. (V1-V6 are really V1R through V6R, on the right chest):
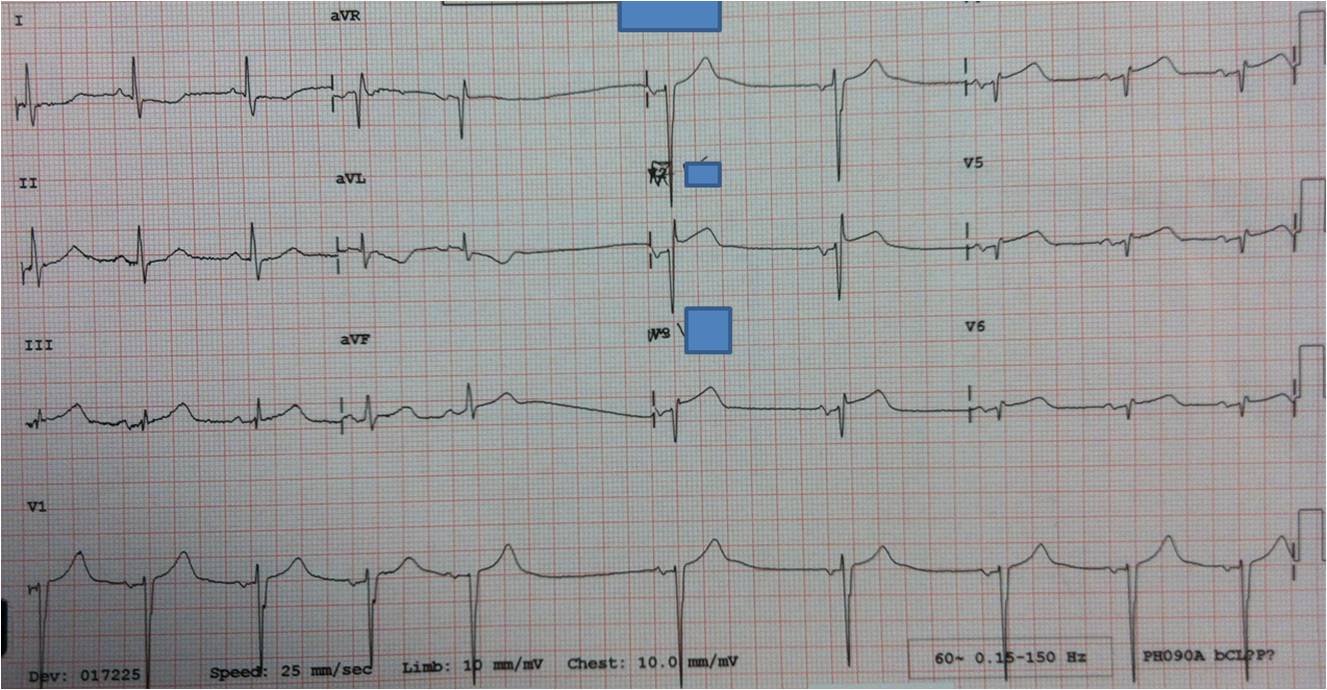 |
| There is ST elevation throughout the right sided leads (V2R-V6R). There is still no ST elevation in inferior leads. Only 0.5 mm is required for the diagnosis of RV MI, with reasonable sensitivity and specificity. Here there is at least 1 mm in V2R through V4R) |
The emergency physician activated the cath lab, and the interventionalist was not convinced but was persuaded to take the patient to the cath lab.
There was a 100% occluded proximal Right coronary artery. It was opened and stented.
12 hour peak troponin I (for what that is worth) was 37 ng/ml.
Here is the post cath ECG:
 |
| Hyperacute T-waves have resolved. Reciprocal ST depression is resolved. There is still minimal ST elevation in V1, which may be the patient’s baseline. The T-waves in V2 and V3 have significantly changed. I do not have enough details of the cath report and anatomy to explain these T-waves in V2 and V3; perhaps they are related to the right ventricular ischemia. |
Lessons:
In our study of inferior MI vs. other etiologies inferior STEMI, 28% had ST depression and T-wave inversion in lead aVL before they had 1 mm of ST elevation in any inferior lead. This case is especially unusual in that no amount of inferior ST elevation was present; the diagnosis relied upon reciprocal findings and right ventricular findings.
I don’t have the whole cath report, nor an echo showing inferior wall motion abnormality. One might argue that this was an RV MI only, without inferior wall involvement (a non-dominant RCA that only supplies the RV). However, there are clearly inferior hyperacute T-waves which resolve, so this is an inferior wall MI.
