Prehospital
A male in his 80s was crossing the street, felt weak, and sat down. He denied LOC, chest discomfort or dyspnea. He had no medical history.
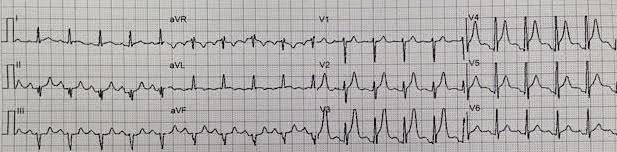
Here is the prehospital ECG (sorry for the poor resolution):
 |
| There is profound ST elevation in anterior leads. 3.5 mm at the J-point in lead V3; 5 mm at 60 ms after the J-point. There is convex ST elevation in aVL, with reciprocal concave ST depression in inferior leads. This is diagnostic of STEMI due to proximal LAD occlusion, especially in an 80 year old. Young men could conceivably have this much precordial ST elevation at baseline, but even in a young man, the limb lead abnormalities make this diagnostic. There is also a large amount of PR depression in V3 and V4, which just goes to show that this finding is NOT specific for pericarditis. |
ED course
He arrived by ambulance stating that he now feels fine.
His exam was unremarkable, including no murmur.
The emergency physician was very concerned about the ST elevation and large T-waves, and activated the cath lab. The interventionalist cancelled it, stating that it does not represent STEMI. The K was 4.0 mEq/L.
The emergency physician then used the early repol/LAD occlusion formula and obtained 24.7.
With STE V3 60 of 5 mm and a computerized QTc 415 ms, and R-wave amplitude of 14, I calculate a formula value of 25.9.
This is very high and just confirms the obvious.
Two more cardiologists came to look at the ECG. Both said “No STEMI.”
I don’t know what they are thinking, but I am not inhibited about speculating: The patient had no chest pain. He only had weakness. Many physicians just cannot accept that a patient with minimal symptoms has anterior STEMI.
Furthermore, many still believe that if there is upward concavity in all of leads V2-V5, it cannot be LAD occlusion or STEMI. There are at least 3 studies refuting this.
Kosuge 1999.
Smith 1 2016.
Smith 2 2012.
Here is a patient I had in which I made the same mistake:
Spontaneous Reperfusion and Re-occlusion – My Bad Thinking Contributes to a Death
In fact, the patient was feeling better and wanted to go home, but the emergency physician convinced him to stay.
The first troponin was below the level of detection.
Here are subsequent ECGs:
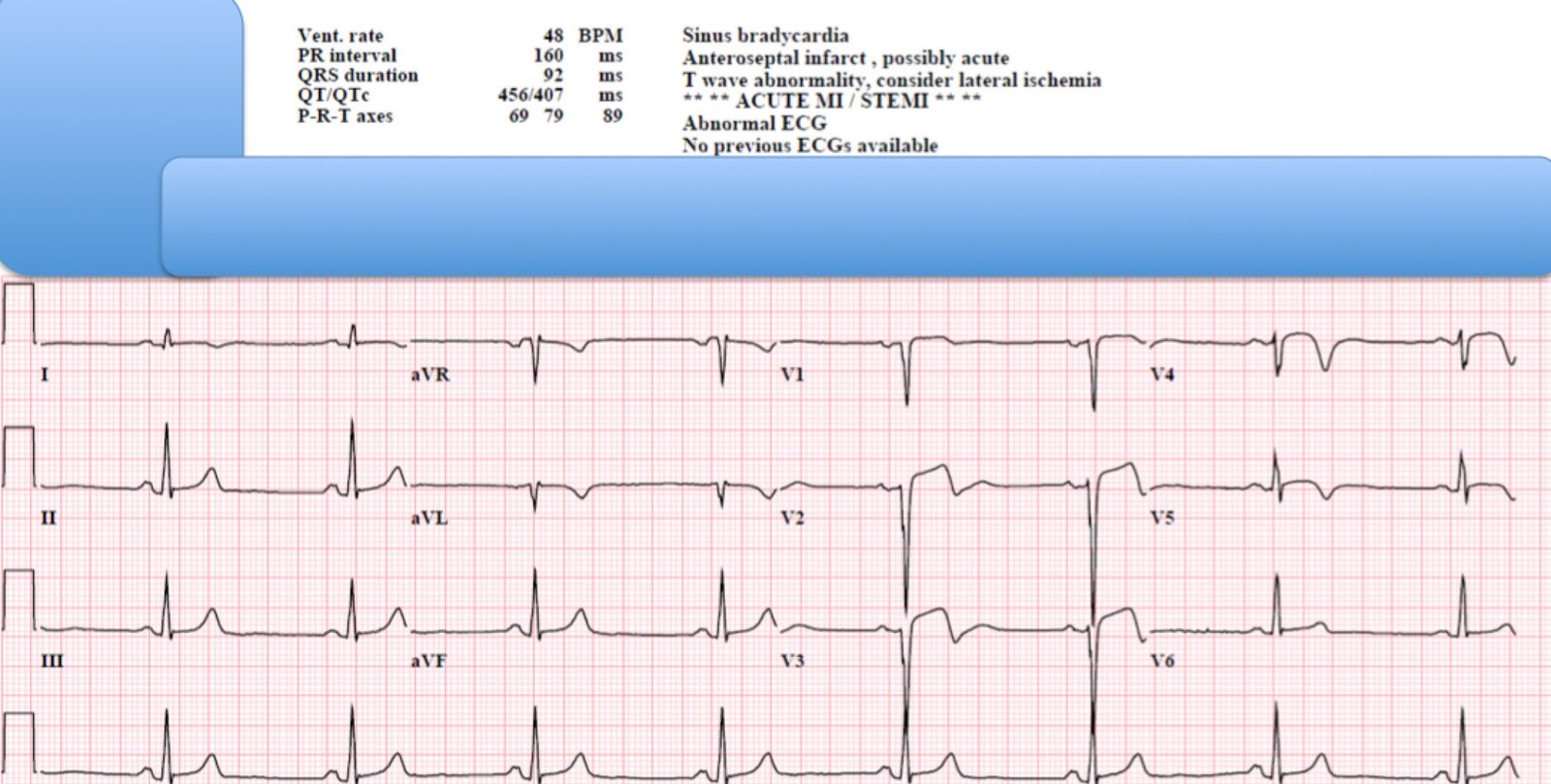
35 minutes after the first:
 |
| T-waves and ST Elevation are much less marked. Limb leads have the same worrisome features. |
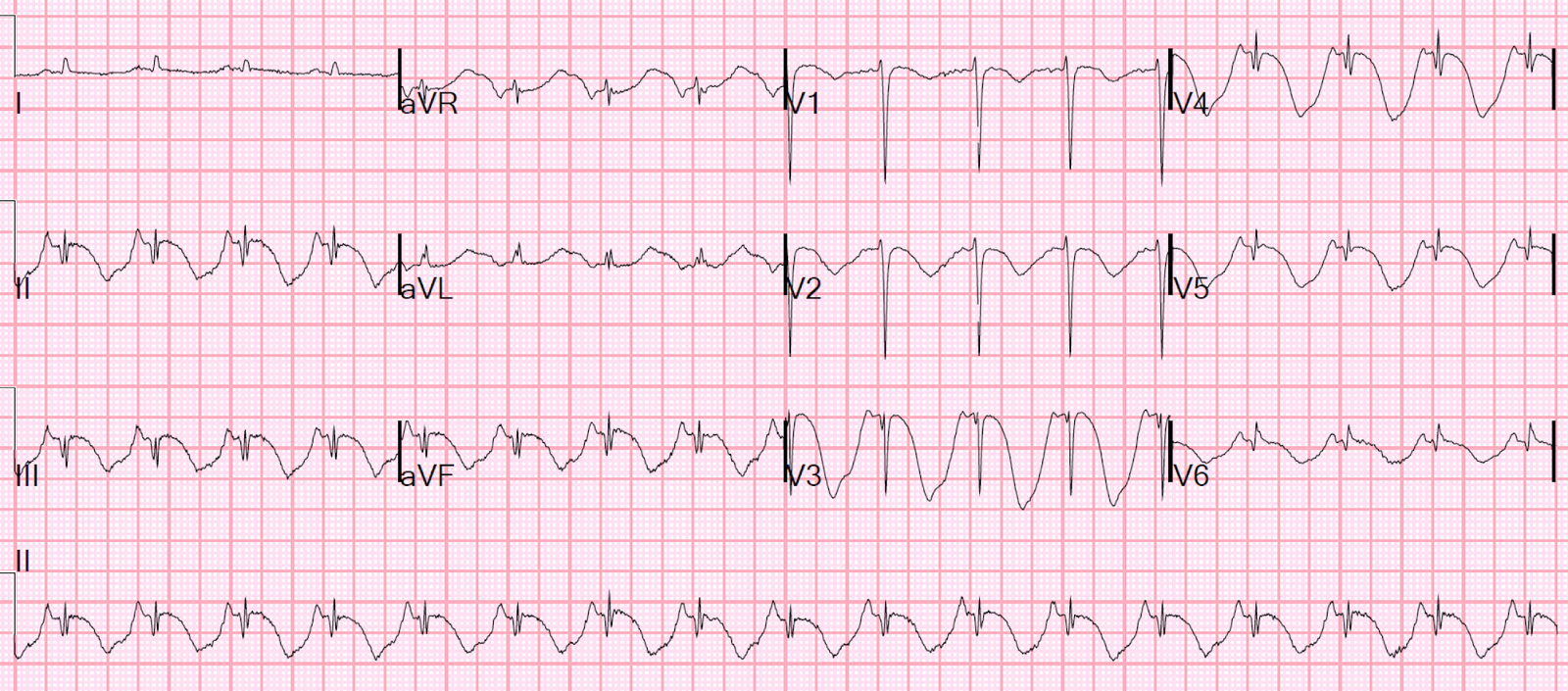
78 minutes after the first:
 |
| There is the beginning of T-wave inversion |
5 hours later:
 |
| More T-wave inversion (consistent with reperfusion). |
A later troponin I was 3.6 ng/mL, but it was not checked after that.
Cath was done the next morning:
EF 45%-50%
Left Main: normal
LAD: 65-70% stenosis (culprit).
severe aortic stenosis
No intervention was done. Patient was transferred for aortic valve replacement and CABG.
Fortunately for this patient, his LAD spontaneously reperfused and remained open, unlike this case of mine which I have already placed a link to above.
Learning Point:
1. Absence of Chest pain means little in the face of a diagnostic ECG.
33% of patients with both NonSTEMI and STEMI have no “chest discomfort”. This was not a study of “chest pain” but of “chest discomfort.”
After patients are diagnosed with MI, they may be browbeaten into saying they had chest pain, or may change their memory. But when the history is taken before the diagnosis, 33% have no chest discomfort.
2. Not all cardiologists are proficient in diagnosing coronary occlusion on the ECG. There are countless things cardiologists must learn, and diagnosing occlusion on the ECG is only one small part of their vast specialty. They are very smart and hard working and knowledgeable, but they, like all people (and like me did in the case above), make mistakes and can suffer from group-think.
Only you can advocate for your patient.