A male in his 50’s called 911 for constant 8/10 midsternal chest pressure. Here was his prehospital ECG:
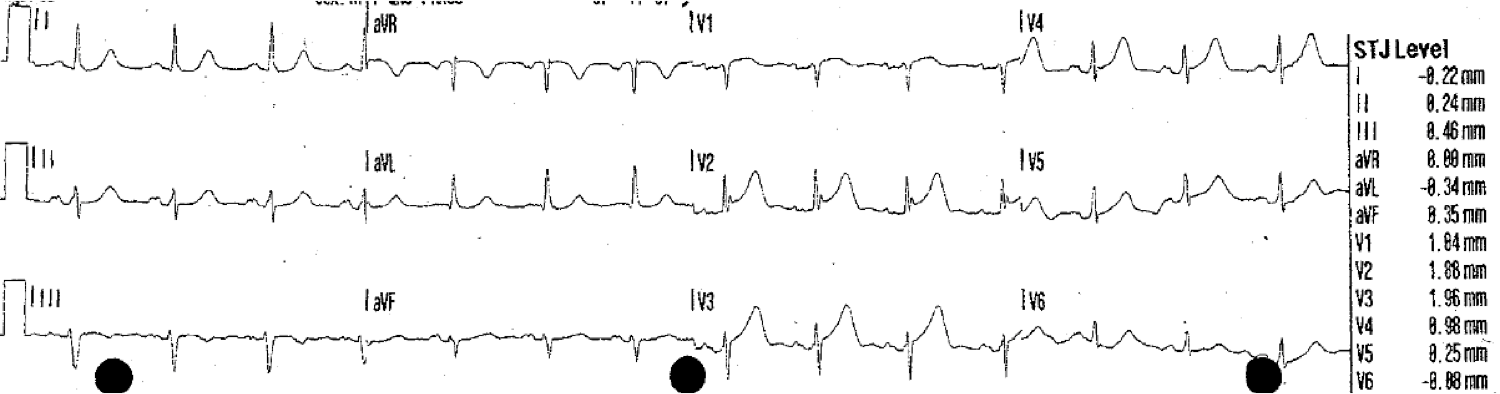 |
| Computerized QTc is 423 ms. The ST elevation at the J-point was measured by the computer (see right side), and is less than the “criteria” for anterior STEMI (2 mm in males over age 40). There is also almost a saddleback morphology in V2. I say “almost” because the R’ wave is not tall enough to be a typical saddleback.
By the 4-variable subtle LAD occlusion vs. Early Repol formula, this is clearly LAD occlusion: STE60V3 = 2, RAV4 = about 7, QRS = 9 mm; value = 20.88 (greater than 18.2 indicates probable LAD occlusion) |
Here is a typical saddleback morphology, which is rarely due to STEMI:
 |
| This saddleback ST elevation prompted a false positive cath lab activation. It was due to LVH.
Notice that there is a significant preceding S-wave Notice the tall preceding R’ wave.
Such saddleback ST elevation is rarely due to STEMI (I have never seen one that was!).
This nearly meets ECG criteria for type 2 Brugada morphology (I will post on that difficult topic soon). Full text link: Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report |
Case continued:
He was given 2 sublingual NTG, with improvement of pain to 4/10. Here was the second prehospital ECG:
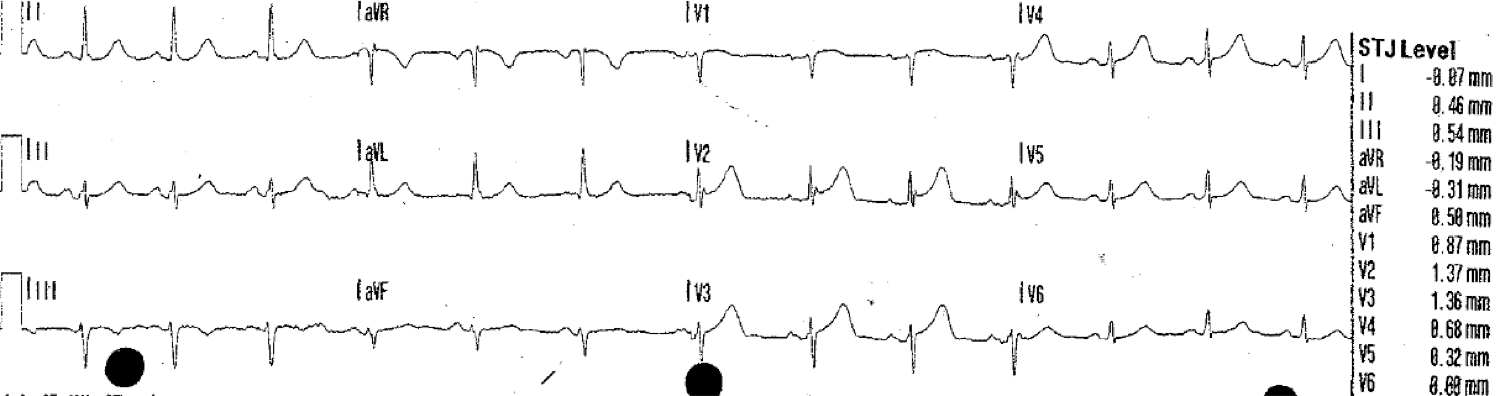 |
| Computerized QTc is 421 ms. There is no significant change. |
He arrived in the ED and had this ECG recorded:
 |
| QTc is 435 ms. There is still less than 2 mm STE at the J-point, so it does not meet STEMI criteria. The formula, using 1.5, 435, and 11 gives a value of 23.8, which, greater than 23.4 is unequivocally positive. LAD occlusion must be assumed until proven otherwise. |
The ECG was read as normal by both the computer and the physician.
Comment: Readers of this blog may be critical of this, but that is because you have been sensitized to this diagnosis. This is the normal assessment throughout the world! To do better than this is the exception, not the norm.
That is why in study after study, 20-30% of angiograms done for “rule-in MI” by troponins find an 100% occluded artery at next day angiogram.
Don’t be critical of this assessment; rather, pass the word and help your fellow emergency physicians and cardiologists to see these findings.
The initial contemporary, sensitive troponin (but not high sensitivity troponin — these are not yet available in the U.S.) was less than 0.10 ng/mL (undetectable).
The first troponin is negative in 50% of acute STEMI.
A repeat ECG was done 140 minutes later:
 |
| QTc is 444 ms. There is no more STE than before. T-waves are slightly different, but not larger. Q-waves are beginning to form in V2 and V3. This proves it is an acute anterior MI. |
A troponin drawn almost 4 hours after the first one was 0.18 ng/mL. It doesn’t sound very high, does it? The Q-waves were not noticed.
Case continued
At 4.5 hours, another ECG was recorded:
 |
| At this point, the Q-waves were noticed and the cath lab was activated. |
A 100% LAD occlusion was stented.
No further followup is available.
Learning point
I repeat this theme over and over: Acute coronary occlusion may be very subtle. It is frequently missed. Readers of this blog probably would not miss this. The person who sent it to me does read the blog, and he was doing QA when he noticed this and immediately recognized that it was a missed subtle occlusion. It would be classified as a NonSTEMI. He states that it is difficult to convey to his colleagues how to recognize these.