This was sent to me with no information (until later).
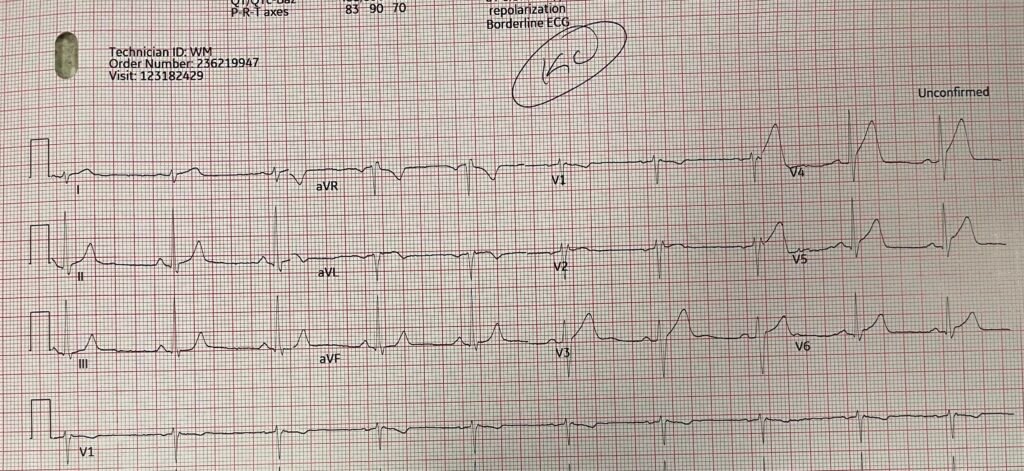
The conventional computer algorithm says “Early Repolarization” The overreading cardiologist said “Early repolarization.”
What do you think?
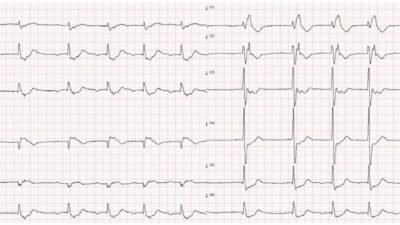
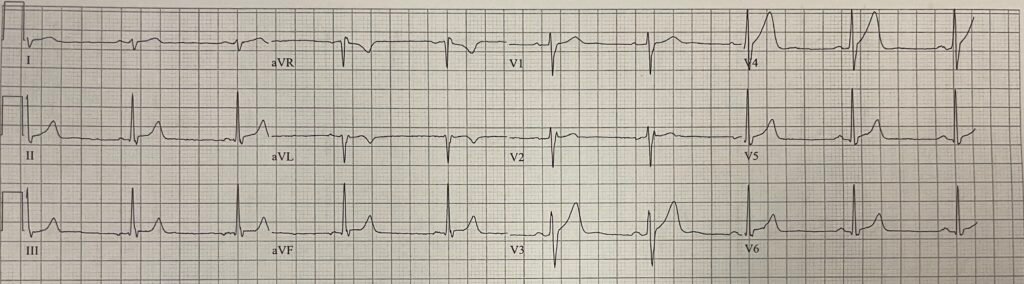
Diagnostic of LAD Occlusion. There is sigificant STE and hyperacute, inflated, T-waves in V3-V6. Moreover, this is clearly a STEMI (+) OMI; there are 3 mm STE in V3 and 2mm in V5: that meets STEMI mm criteria. One would think that OMI that meet STEMI criteria would be easily diagnosed by physicians. There is very little good data on this, but anecdotal evidence suggests that MANY cases of OMI that meet STEMI criteria are diagnosed as early repolarization
Here is the history:
48 year old male smoker 135 pounds, dancing, performing, classic CP, sweating, presents 45 minutes after the onset of chest pain. Pain decreased from 8/10 –> 4/10 after nitro.
The sender immediately diagnosed LAD OMI.
I later put it through the PMCardio Queen of Hearts. The Queen obviously had no problem with this ECG:
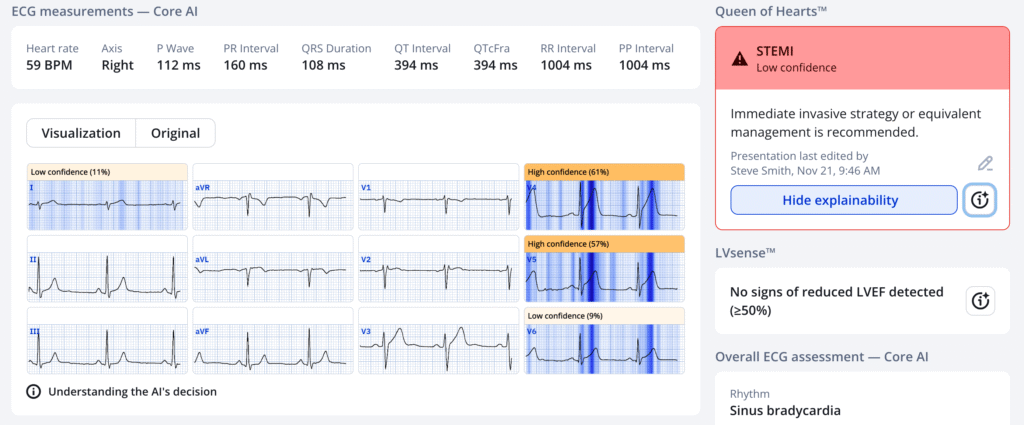
PMcardio for Individuals now includes the latest Queen of Hearts model, AI explainability (blue heatmaps), and %LV Ejection Fraction. Download now for iOS or Android: https://individuals.pmcardio.com/app/promo?code=DRSMITH20. As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA.
The sender is not at a PCI center. It is a prolonged transport, so he must give thrombolytics to OMI.
The sender immediately gave TNK-tPA with a door to drug time of 14 minutes. After lytics, pain completely resolved within minutes.
This is the ECG recorded 19 minutes after lytics were administered:
This shows reperfusion. Now you could actually diagnose “early repolarization” if you saw this in isolation!! (In fact, the Queen says “Not OMI” with absolute certainty). Where there was STE, it is now diminished: In V4, from 3mm to 1mm; in V5, from 2mm to 0.5mm; in V6, from 1 mm to 0.5mm. Also, the T-wave is not as fat (not hyperacute).
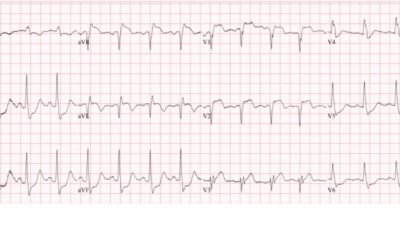
Another ECG 11 minutes later, at 30 minutes after TNK, was recorded:
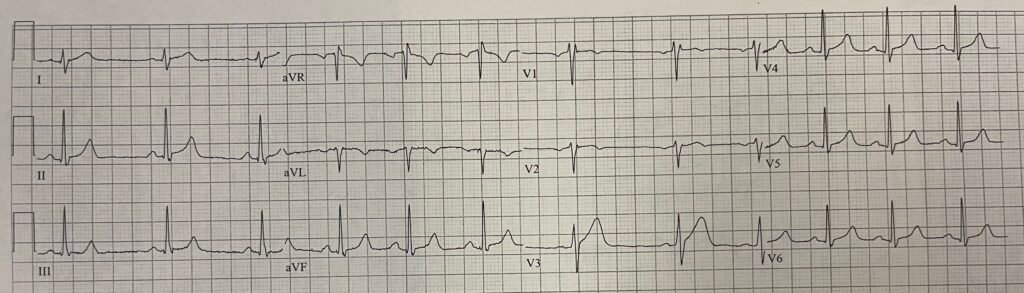
Now there is slightly less STE in lead V3. The T-waves are far smaller (lower amplitude, far less area under the curve, less symmetric). The “inflated” Hyperacute T-waves on the first ECG have “deflated”.
The first troponin I returned at 0.082 ng/mL.
“Rescue PCI” after failed thrombolytics is done if there is absence of good evidence of reperfusion. The ECG is the evidence. If there is >70% resolution of STE, that is considered definite reperfusion.
From Open Evidence: This threshold is supported by multiple studies and guidelines, which show that complete (≥70%) ST-segment resolution is a reliable marker of successful myocardial reperfusion and is associated with improved outcomes.[1-3] Partial resolution (30–70%) or no resolution (<30%) indicates incomplete or failed reperfusion and is associated with larger infarct size and worse prognosis.[3] The American College of Cardiology/American Heart Association guidelines recommend rescue PCI in patients with STEMI who have evidence of failed reperfusion after fibrinolytic therapy, which is most commonly determined by persistent ST-segment elevation and ongoing symptoms.[4]
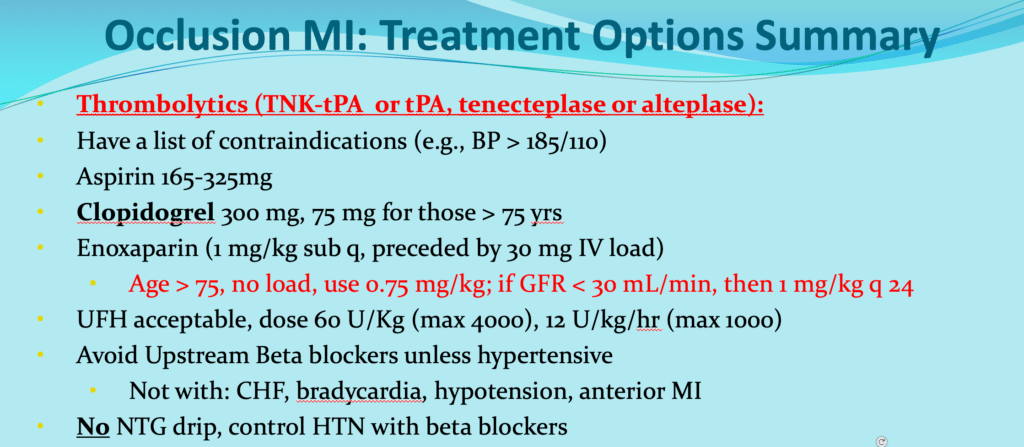
Aside: when giving TNK-tPA, one should also give 300mg of clopidogrel. Enoxaparin is the preferred anticoagulant, and is given with an IV load (lower dose for age > 75). See total summary here:
Early after onset of occlusion, thrombus is fresh and thrombolytics are VERY effective. Some studies say that they are more effective than PCI in the first hour or two. Guidelines nevertheless always recommend PCI if door in, door out, door in to balloon time is less than 90 minutes, or if first medical contact by EMS to balloon time is less that 120 minutes. This is largely because of the risk of intracranial hemorrhage in thromobolytics, which is at least 1% even among the lowest risk group.
These short times are hardly ever achieved in any transfer system, so err towards giving thrombolytic if you need to transfer.
See CAPTIM trial below for data on thrombolytics early after onset of chest pain
Follow up:
Because there was reperfusion, PCI could be done the next day
There was a 50% stenosis of LAD, with thrombus, managed medically.
This brings up another interesting debate: do most MIs occur in stenotic lesions that are <50% at baseline? Many older studies found this, but more recent data indicates that atheromatous lesions progress rapidly in the months prior to OMI, such that about 84% are >50% at the time they rupture and thrombose. But that means that 16% are <50%.
CAPTIM trial in Circulation 2003:
Steg PG, Bonnefoy E, Chabaud S, et al. Impact of time to treatment on mortality after prehospital fibrinolysis or primary angioplasty: data from the CAPTIM randomized clinical trial. Circulation [Internet] 2003;108(23):2851–6. Full text: https://www.ahajournals.org/doi/pdf/10.1161/01.cir.0000103122.10021.f2
Background—CAPTIM was a randomized trial comparing prehospital thrombolysis with transfer to an interventional facility (and, if needed, percutaneous intervention) with primary percutaneous coronary intervention (PCI) in patients with ST-segment–elevation myocardial infarction (STEMI). Because the benefit of thrombolysis is maximal during the first 2 hours after symptom onset, and because prehospital thrombolysis can be implemented earlier than PCI, this analysis studied the relationship between the effect of assigned treatment and the time elapsed from symptom onset.
Methods and Results—Randomization within 2 hours (n460) or 2 hours (n374) after symptom onset had no impact on the effect of treatment on the 30-day combined primary end point of death, nonfatal reinfarction, and disabling stroke. However, patients randomized <2 hours after symptom onset had a strong trend toward lower 30-day mortality with prehospital thrombolysis compared with those randomized to primary PCI (2.2% versus 5.7%, P=0.058), whereas mortality was similar in patients randomized >2 hours (5.9% versus 3.7%, P=0.47). There was a significant interaction between treatment effect and delay with respect to 30-day mortality (hazard ratio 4.19, 95% CI 1.033 to 17.004, P0.045). Among patients randomized in the first 2 hours, cardiogenic shock was less frequent with lytic therapy than with primary PCI (1.3% versus 5.3%, P0.032), whereas rates were similar in patients randomized later.
Conclusions—Time from symptom onset should be considered when one selects reperfusion therapy in STEMI. Prehospital thrombolysis may be preferable to primary PCI for patients treated within the first 2 hours after symptom onset. (Circulation. 2003;108:2851-2856.)
So the study was underpowered to show that lytics are better than PCI if given very early after chest pain onset.
= = =
======================================
MY Comment, by KEN GRAUER, MD (12/9/2025):
As per Dr. Smith — Management in today’s case can (and should) be quickly decided because: i) The history is classic for acute cardiac CP (Chest Pain); — ii) In the context of this history, the initial ECG is diagnostic of an acute OMI; — and, iii) Prompt PCI is not available within the area where this patient presented — therefore prompt institution of thrombolytic therapy is the appropriate alternative that should be immediately instituted.
= = =
Why is today’s Initial ECG Diagnostic of an Acute OMI?
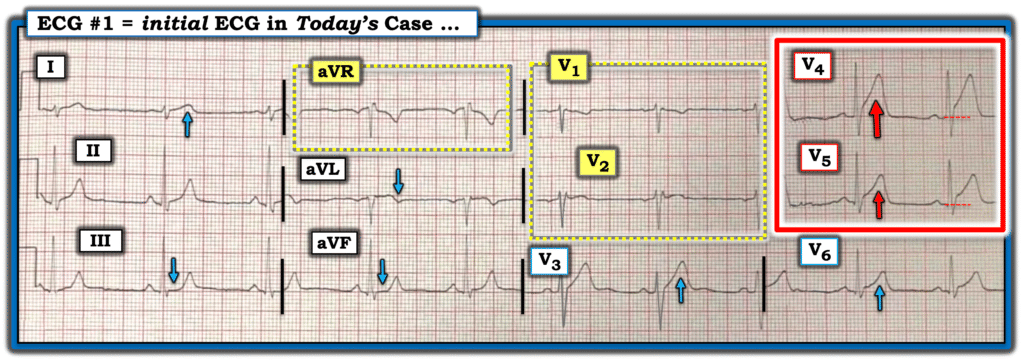
For clarity in Figure-1 — I’ve reproduced and labeled today’s initial ECG.
- In this middle-aged man who presented with typical new-onset CP — My “eye” was immediately drawn to lead V4 (within the RED rectangle). Not only is there at least 2 mm of ST elevation — but this ST-T wave is clearly hyperacute in this clinical context (much taller and “bulkier”-than-expected — with an extremely wide base).
- The T wave in neighboring lead V5 (also within the RED rectangle in Figure-1) is not quite as tall as in lead V4 — but otherwise manifests similar hyperacute features of ST segment straightening and elevation with a “fatter”-than-expected and similarly widened T wave base.
- Given these obvious abnormalities in leads V4,V5 — neighboring leads V3 and V6 manifest lesser, but nevertheless still hyperacute features (ie, the “bulky” T wave in lead V3 dwarfs the R wave in this lead).
- NOTE: The lead V1 and V2 electrodes were almost certainly placed too high on the chest because: i) Both of these leads manifest a terminal r’ (which is uncommon in V1 and highly unusual in lead V2); — ii) Both leads V1 and V2 manifest terminal negativitiy of the P wave; — and, iii) QRS morphology of both leads V1 and V2 resembles the QRS appearance in lead aVR. In addition — the T wave in lead V1 is negative — and the only reason the T wave in lead V2 is not negative, is that there would doubtless otherwise be continuation of the hyperacute ST elevation that we see in leads V3-thru-V6 (See our page on Technical Misadventures for numerous examples of leads V1,V2 misplacement).
- The reason recognition of lead V1,V2 misplacement is relevant in today’s case is our finding of hyperacute T waves beginning with lead V3. I strongly suspect that with proper V1,V2 placement — ST elevation consistent with acute proximal LAD occlusion would also be seen in leads V1,V2.
- Finally — subtle-but-real ST-T wave findings are also seen in the limb leads (a hyperacute T wave in lead I, given how tiny the QRS [and especially the R wave] in lead I is — subtle ST elevation with T wave inversion in lead aVL — and ST segment flattening in leads III,aVF with terminal T wave peaking in all 3 inferior leads).
= = =
Figure-1: Todays initial ECG.
= = =
= = =