Written by Magnus Nossen
Today’s patient is a 50-something male with a history of mechanical aortic valve due to aortic insufficiency. He is otherwise healthy except for hypertension. The patient experienced sudden onset palpitations while at home watching TV. When symptoms did not subside, he called EMS.
The ECG below was recorded on scene by the paramedics. Except for tachycardia, the patient’s vital signs were normal and he denied any chest pain. What do you think? How would you handle this patient?
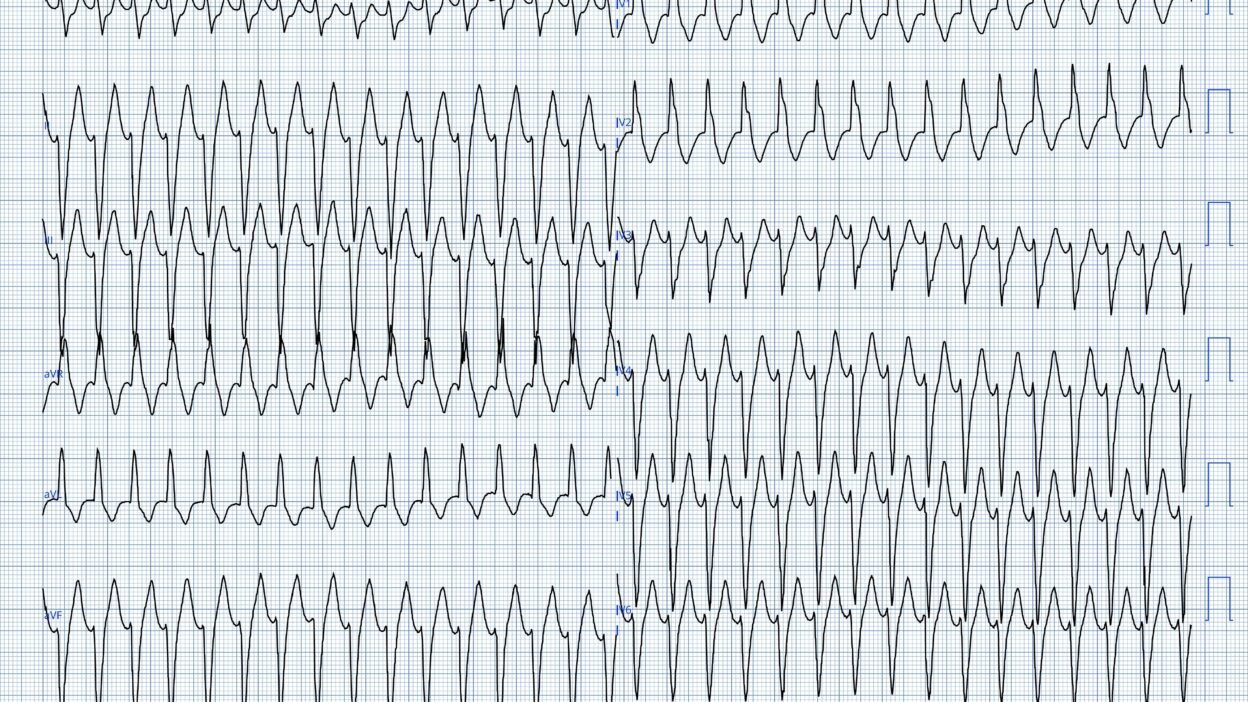
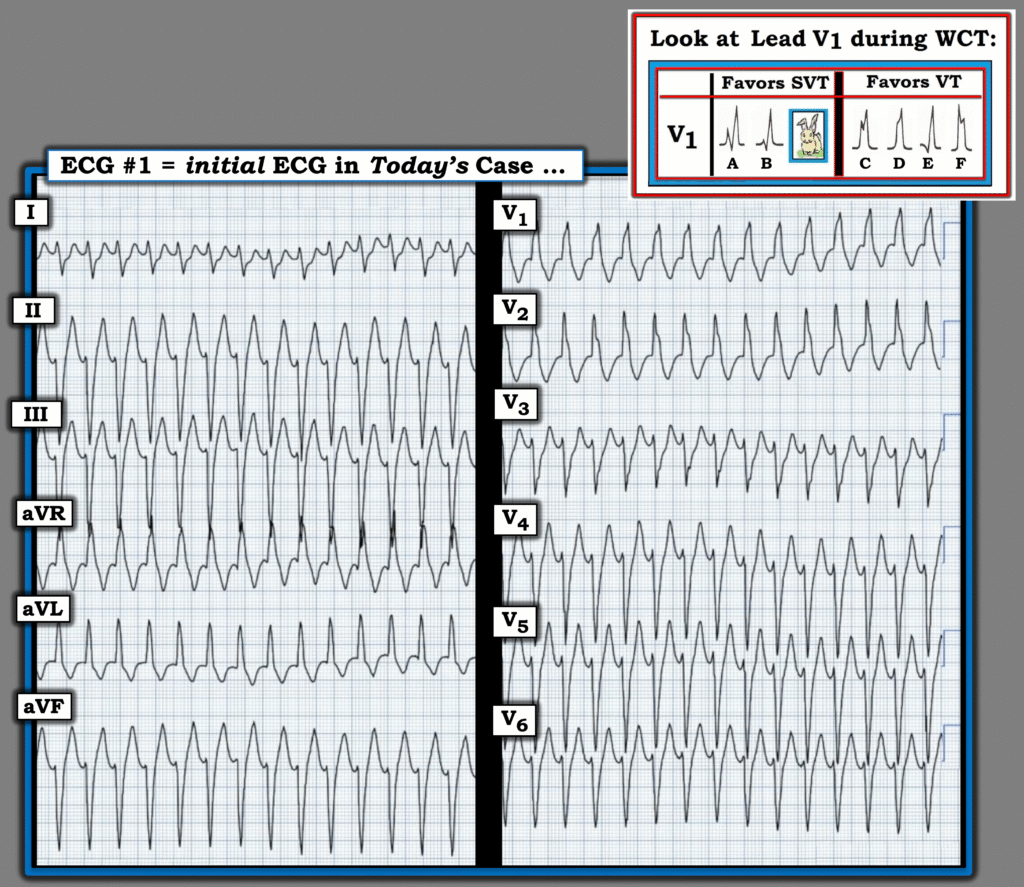
ECG #1 recorded by EMS

The ECG shows a wide-complex tachycardia at 177 beats per minute. The QRS morphology is consistent with right bundle branch block and left anterior fascicular block pattern. QRS duration 132ms.
The patient was assessed as hemodynamically stable by EMS. He was transported to the emergency department by ambulance.
How would you manage this patient?
Smith: Of course, electricity is usually the best option for a tachydysrhythmia. However, this patient is stable and it is not required to emergently cardiovert. One can take a bit of time to think.
So what do you think?
Magnus: I sent ECG #1 to Dr Smith who instantly wrote back: “posterior fascicular VT”. This was my impression as well.
Smith: You can never be abolutely certain that the ECG represents posterior fascicular VT. If you are mistaken, and give verapamil to a patient with, for instance, scar-mediated VT, it can be disastrous. So how can you be certain that verapamil is safe? Do a bedside ultrasound. Because PFVT is not due to pathologic myocardium, the EF should be relatively normal. And Verapamil is safe when the EF is normal. So I would do a bedside echo and, if the EF is good, give verapamil.
What actually happened?
In the ED, the arrhythmia spontaneously terminated without any intervention. Echocardiography showed a normally functioning mechanical aortic valve and no evidence of wall motion abnormalities. The ejection fraction was normal and INR was within the therapeutic range.
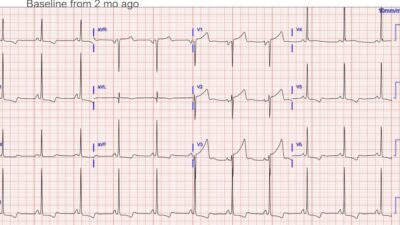
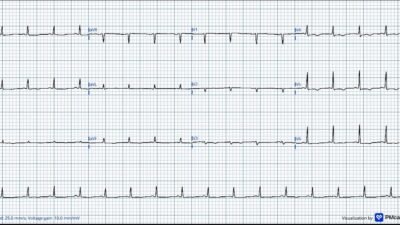
ECG #2 recorded in the ED
ECG recorded after termination of arrhytmia. Standard lead lay out. This ECG shows sinus rhythm 67min. PR interval is normal at 182ms QRS complexes are narrow at 105ms. There are no signs of ischemia. This ECG was unchanged from prior.
How would you manage this patient going forward?
Case continuation:
The patient was admitted for VT work-up. Coronary angiography was performed the following day due to a mild elevation in troponin levels. The patient had no history of chest pain and denied any symptoms suggestive of angina. The angiogram demonstrated normal coronary arteries, and the minor troponin elevation was attributed to the tachycardia itself, consistent with a type II myocardial injury mechanism.
The treating physicians did not recognize the ECG pattern as consistent with fascicular VT. Medical treatment with a beta blocker was initiated. Over the next couple of months the patient had many visits to the ED and cardiology department due to episodes of palpitations. He continued to experience recurrent episodes of ventricular tachycardia, and several anti-arrhythmic medications including metoprolol, amiodarone, and sotalol were tried in succession without effect. After failed medical therapy the patient had an ICD implanted.
ICD implantation will off course not fix the problem. An ICD can only help terminate arrhythmia via anti-tachycardia-pacing or DC shock. Continued perscription of amiodarone in our patient slowed the VT rate leading to persistent VT below the detection rate of the ICD.
Eventually, after months of trying to treat the arrhythmia with conventional anti-arrhythmics (which was unsuccessful), the patient was referred for VT ablation.
This should have been done after the initial hospitalization!
Not surprisingly a posterior fascicular VT was identified and ablated. Had the fascicular VT pattern been recognized during the initial hospitalization, this patient would likely have avoided months of recurrent VT, unnecessary exposure to amiodarone and ICD implantation. Fascicular VT was never mentioned in the chart prior to the electrophysiological study and ablation procedure and neither was verapamil.
Posterior fascicular VT is the most common fascicular VT. Originating in the left posterior fascicle, QRS complexes show RBBB and LAFB pattern. It is characterized by ralatively narrow QRS complexes (<140ms) with a short RS interval (60-80ms).
Posterior fascicular VT is one of the idiopathic VT subtypes. It usually responds poorly to conventional antiarrhytmics used for scar mediated VT (beta blockers and amiodarone). However, this type of arrhthymia almost invariably responds well to verapamil. Verapamil is great for both termination of ongoing arrhythmia and for prevention of recurrence.
Idiopathic VT is classically described in patients with a structurally normal heart. Strictly speaking, prior aortic valve replacement places this patient outside that category. However, in this case coronary angiography ruled out coronary artery disease and echocardiography showed no cardiomyopathy or myocardial scar. There was preserved biventricular function, and a well‑functioning mechanical aortic valve. There is no reason to think this arrhythmia has anything to do with the prior aortic valve replacement. Had I been responsible for the patient’s care, I would have started verapamil and referred the patient for electrophysiological study with a view to catheter ablation
Smith: This illustrates why electricity is often NOT the answer, especially for posterior fascicular VT. This dysrhythmia often recurs. As Magnus writes, had the patient been correctly diagnosed initially, he could have received verapamil and avoided all these complications.
Here is another case that illustrates this problem: Incessant Regular Wide Complex Tachycardia
Read this post: Idiopathic Ventricular Tachycardias for the EM Physician
Learning points:
- Fascicular VT typically responds poorly to standard antiarrhythmics, but is characteristically sensitive to intravenous verapamil, which often terminates the tachycardia rapidly.
- Idiopathic ventricular tachycardias typically occur in otherwise healthy individuals.
- This case highlights that even though there is a history of cardiac disease, it is sometimes reasonable to consider idiopathic VT as the cause of WCT.
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/9/2026):
Today’s case by Dr. Nossen serves as an important reminder of KEY considerations for assessing the patient who presents with a regular WCT (Wide-Complex Tachycardia) when there is no clear sign of sinus P waves.
- I focus my comments on some additional considerations to those put forth in Dr. Nossen’s discussion.
= = =
Idiopathic VT:
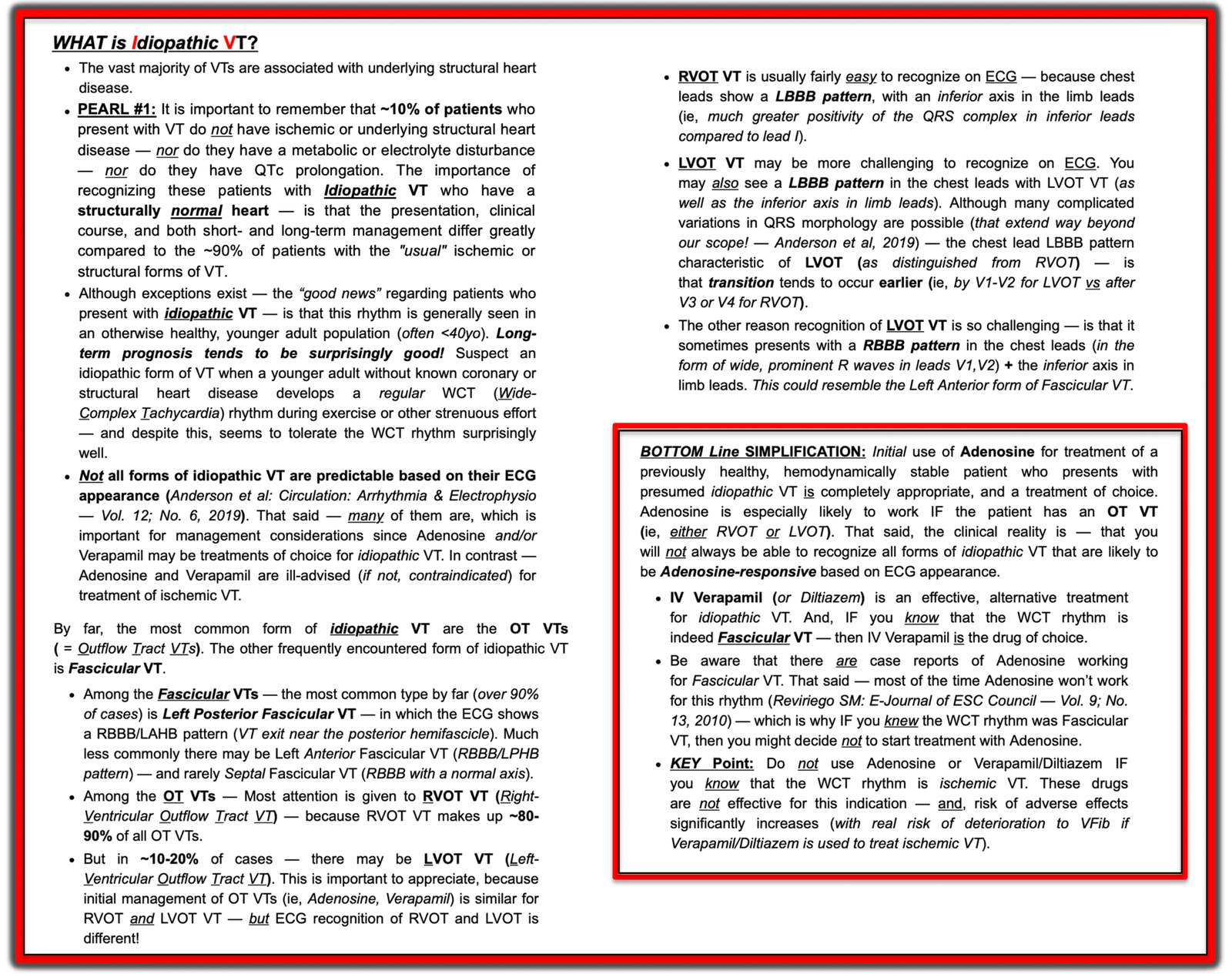
As we’ve periodically reviewed in Dr. Smith’s ECG Blog — Idiopathic VT is a special form of ventricular tachycardia, in which the patient does not have underlying structural heart disease (See My Comment — at the bottom of the page in the July 5, 2025 post).
- Depending on the population surveyed — one of the forms of idiopathic VT make up ~10% of all VTs seen in practice. However, among previously healthy, younger adults — a much greater percentage of VT rhythms will turn out to be idiopathic VT.
- In contrast — the prevalence of idiopathic VT is much less among older adults with underlying heart disease, in whom the great majority of VT rhythms are ischemic or structural in etiology.
- Appreciation of these differences in VT prevalence impacts the relative likelihood that a regular WCT rhythm will turn out to be supraventricular vs some form of VT. Statistical likelihood that a regular WCT rhythm in an older adult with heart disease will turn out to be VT is at least 90% (with most of these VTs being of ischemic or structural etiology).
- In contrast, among a population of previously healthy younger adults who present with a regular WCT — idiopathic VT (and not SVT with aberrant conduction) will be found much more often than is generally appreciated.
- As I summarize below in Figure-1 (and in my 8-minute Audio Pearl that appears in the Addendum below) — the clinical significance of distinguishing idiopathic VT forms (ie, in patients who do not have underlying heart disease) — from ischemic and structural VT forms (that make up the vast majority of VTs in older patients with heart disease) — is that evaluation and treatment are very different, with in general a much better longterm outcome and response to treatment with the idiopathic VTs.
= = =
KEY“Take-Home” Point: Both in younger and older adult populations — VT occurs more commonly that many clinicians appreciate. As a result — we need to always consider the possibility of VT in any patient who presents with a regular WCT rhythm without clear sign of sinus P waves.
- The above KEY point holds true regardless of whether or not the patient is hemodynamically stable! While patients with sustained VT are much more likely to decompensate than those who remain in a persistent SVT rhythm (especially when the patient is older and has underlying heart disease) — this generality does not always hold true. Some patients in sustained VT remain hemodynamically stable for hours — or even longer (with documentation of occasional cases of sustained VT having persisted for days — with providers around the bedside refusing to believe this to be possible).
- Especially with forms of idiopathic VT (in which the patient does not have underlying heart disease) — sustained VT may persist for surprisingly long periods of time. Therefore — Hemodynamic stability can not be used to rule out VT!
= = =
How to distinguish Idiopathic VT from SVT?
Aberrant conduction most often presents as rate-related QRS widening that manifests a QRS morphology that resembles some form of known conduction defect (ie, either RBBB, LBBB, LAHB, LPHB, or RBBB with a hemiblock). This is because the refractory periods of the various conduction fascicles are not the same. In most patients — the refractory period of the right bundle branch tends to be the longest, which is why RBBB conduction is the most common form of rate-related aberrancy. But any conduction pattern may be possible with rate-related aberrancy.
- On rare occasions — “something else” (ie, hyperkalemia, sodium channel blocker toxicity — or other toxicity) may result in a regular WCT rhythm, especially if the QRS is extremely wide (more than 0.14 second). That said — in a previously healthy younger adult (assuming no WPW-related arrhythmias) — the main consideration is to distinguish between VT vs SVT with either preexisting BBB or rate-related aberrant conduction.
- QRS morphology may allow for greater precision in predicting WCT etiology — especially if ECG features predictive of either VT or SVT are present. That said, even in cases in which QRS morphology is suggestive — it is rare to attain 100% certainty prior to our need to begin treatment.
- Much (most) of the time — we will need to begin treatment before we are certain of the diagnosis. Remember that if at any time during the process, the patient shows signs of becoming hemodynamically unstable — that synchronized cardioversion is immediately indicated. That said, in the absence of diagnostic certainty — empiric treatment based on our best hunch diagnosis is reasonable.
As discussed below in Figure-1 — fascicular VT is one of the most common forms of idiopathic VT.
- Because of its origin near the left anterior or the left posterior hemifascicle — QRS morphology with fascicular VT resembles either RBBB/LAHB or RBBB/LPHB conduction.
- The above said — my favorite clue that a WCT rhythm may turn out to be fascicular VT — is that there are some atypical ECG features of either RBBB or of hemiblock conduction!
= = =
Figure-1: Review of KEY features regarding idiopathic VT.
= = =
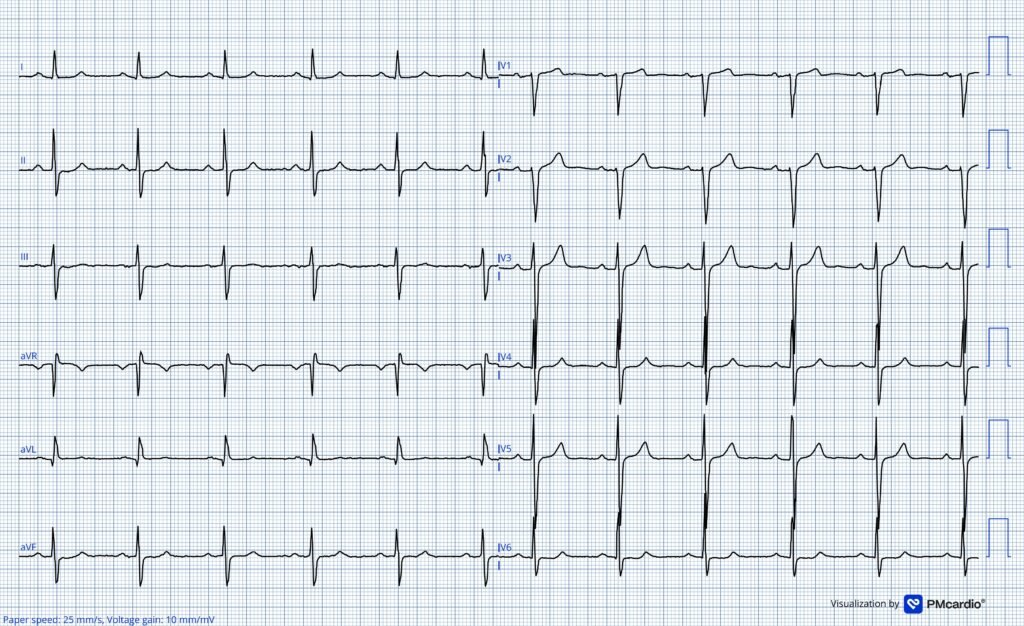
Back to Today’s CASE:
For clarity in Figure-2 — I’ve reproduced today’s initial ECG. To this — I’ve added an insert in the upper right of this figure relating to QRS morphology clues to the WCT etiology.
- As per Dr. Nossen — the ECG in Figure-2 shows a regular WCT at ~175/minute, without clear sign of atrial activity. QRS morphology in this tracing superficially resembles RBBB/LAHB conduction.
= = =
QUESTION: Why then did both Drs. Smith and Nossen immediately recognize today’s ECG as highly suggestive of idiopathic VT?
= = =
Figure-2: Today’s initial ECG — with an insert regarding QRS morphology in lead V1 that favors VT vs SVT.
= = =
Idiopathic VT: Looking for QRS Morphology CLUES . . .
Although exceptions exist — one would expect rate-related aberrant conduction to manifest a more typical QRS morphology for some form of conduction block in an otherwise healthy younger adult. In contrast, in an older adult with underlying heart disease — a less typical QRS morphology becomes likely, even when the rhythm is supraventricular (ie, “scar” from ischemic heart disease and/or cardiomyopathy being more likely to alter QRS morphology).
= = =
Reasons why Drs. Smith and Nossen immediately recognized idiopathic VT for today’s initial ECG include the following:
- With typical RBBB conduction — there is a distinct triphasic rsR’ complex in right-sided lead V1 (with taller right rabbit ear — and S wave that descends below the baseline — consistent with A or B in the insert in Figure-2).
- Instead — QRS morphology in lead V1 is more atypical than I’d usually expect for a supraventricular rhythm (ie, in a patient without underlying coronary disease or cardiomyopathy). This is because instead of a triphasic QRS in lead V1 — we see a monophasic all upright R wave in lead V1 (that most closely resembles pattern D in the insert in Figure-2).
- PEARL: For practical purposes — the only QRS morphology with high specificity for SVT is the presence of the above described morphology that is shown in A or B in Figure-2. While other patterns in the insert are not necessarily diagnostic of VT — any other QRS morphology (ie, C,D,E,F in Figure-2) will increase the likelihood of VT.
The other characteristic feature of RBBB conduction — is the presence of wide terminal S waves in left-sided leads I and V6. Although this is present in Figure-2 — there are other subtle findings in today’s tracing that are less typical of supraventricular conduction:
- Transition in the chest leads to a predominantly negative QRS complex occurs much sooner than I would expect with RBBB conduction (ie, Already by lead V3 — the QRS has become predominantly negative — and it stays predominantly negative throughout the remainder of the chest leads!). Usually with RBBB conduction — there will be more positive activity than what we see here after lead V3 (and it is distinctly uncommon to see no more than the tiny initial r wave that we see here in lead V6).
- Usually with LAHB conduction — there is more of an initial positive deflection in the inferior leads than what we see in Figure-2 (which shows initial r waves that are less than 2 mm in leads II,III,aVF).
- Usually with LAHB conduction — there is a taller R wave in lead I — rather than the predominantly negative complex that we see in Figure-2 (ie, The indeterminate frontal plane axis that we see in Figure-2 is common with fascicular VT — but uncommon with supraventricular rhythms).
BOTTOM Line: Because of all of the above atypical features for RBBB/LAHB conduction — I also immediately suspected fascicular VT for today’s initial rhythm.
- As per Dr. Nossen — IV Verapamil (or Diltiazem) is highly effective for treating fascicular VT — and should have been the agent of choice for treating today’s initial rhythm.
- The “good news” — is that IV Verapamil is also highly effective for treating reentry SVT rhythms (AVNRT, AVRT) — such that this drug would probably have worked regardless of the etiology of today’s WCT rhythm.
- KEY Point: The main caution against using IV Verapamil or Diltiazem to treat a regular WCT rhythm — is that if the rhythm turns out to be an ischemic form of VT — then the negative inotropic and vasodilating effect of these medications may result in patient decompensation. As a result — IV Verapamil (or Diltiazem) should not be given to patients if an ischemic or structural form of VT is more likely (ie, to an older patient with underlying heart disease).
- Regarding today’s case — the not excessively wide QRS and the very typical QRS morphology consistent with fascicular VT in this patient who was not felt to have underlying coronary disease would have justified a trial of IV Verapamil.
= = =
= = =
ADDENDUM:
- NOTE #1: Below is my 8-minute ECG Audio PEARL on Idiopathic VT.
- = = =
- NOTE #2: Below is my 12-minute ECG Audio PEARL on distinction between VT vs SVT when confronted with a regular WCT rhythm. (To Remember — Statistical likelihood that a regular WCT rhythm will turn out to be an idiopathic form of VT will be more than many clinicians appreciate if the patient is a previously healthy younger adult).
- = = =
- For another WCT relevant to today’s case — CLICK HERE —
- = = =
- NOTE: I have been adding selected short ECG Videos on arrhythmia interpretation — that can be found in the TOP Menu on any page in Dr. Smith’s ECG Blog — CLICK HERE — if interested — 🙂
= = =
= = =