Written by Matt McArthur, edited by Jesse McLaren
ED Triage nurse comes to me and asks to look at the ECG of a 50 year old patient. They came in because of progressive SOB over a few days plus some ongoing nausea, chest and back pain. Otherwise healthy with no significant medical history, no asthma/COPD or heart disease, normal body habitus. Triage vitals included HR of 100, BP 140/100, SpO2 100%, and the patient was not ill appearing or distressed.
What do you think?

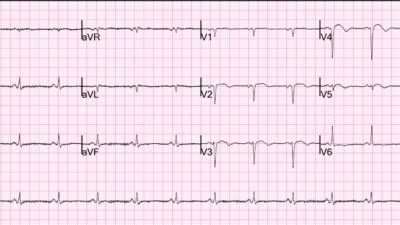
There’s sinus tachycardia with diffuse low voltages across the limb leads (all <5mm) and chest leads (all <10mm), and non-specific T wave inversion V3-5. This is worrisome for pericardial effusion given the history of unexplained dyspnea, tachycardia, and no other known reason for patient to have such low voltages.
I looked at the ECG and told the triage nurse that based on this ECG I was worried the patient had a large/symptomatic pericardial effusion until proven otherwise. I brought POCUS and immediately confirmed this diagnosis at the initial bedside assessment.

These still POCUS images (subxiphoid on the left, and apical 4 on the right) show a large circumferential pericardial effusion. The video images (not shown) showed tamponade physiology with RV/RA diastolic collapse and a noncollapsing IVC, as well as small bilateral pleural effusions.
Further history revealed the patient had been well until 3-4 weeks prior when they experienced a new onset of mid back and chest pain. They went to a walk in clinic and was told it was likely MSK and advised to take tylenol/NSAIDs. The pain persisted. Then the patient began to experience SOB, exertional intolerance, and presyncope, progressive over 3 days which prompted the presentation to ED.
High sensitivity troponin was undetectable (<2). BNP was elevated at 1000 (normal <221). CRP elevated at 110.
The patient was urgently transferred to a nearby cardiac centre and had a pericardial drain placed with 800cc of yellow fluid drained. Final diagnosis was idiopathic pericarditis complicated by pericardial effusion with tamponade.
So the patient had tamponade despite normal blood pressure and no electrical alternans. This is not surprising, as the classic clinical triad for tamponade (hypotension, distended neck veins and muffled heart sounds) has low sensitivity—with the majority lacking hypotension. In addition, the ‘classic ECG triad’ for tamponade (sinus tach + low voltage + electrical alternans) has low sensitivity for tamponade, with the majority lacking electrical alternans.
Learning points
1. The classic clinical triad (hypotension, distended neck veins and muffled heart sounds) and classic ECG triad (sinus tach + low voltage + electrical alternans) have low sensitivities for tamponade
2. Short of breath with sinus tach + low voltage = tamponade until proven otherwise: POCUS to assess for pericardial effusion and tamponade
3. Smith: In our department, every patient with chest pain and/or SOB gets a bedside cardiac ultrasound, so that the diagnosis of effusion/tamponade will be made even without the ECG. But the echo is not done nearly as soon after presentation as the ECG. And so the ECG, recorded immediately at triage, leads to very fast diagnosis.
See other tamponade cases:
- An elderly patient with shortness of breath and near syncope
- Acute chest pain and ST elevation. CT done to look for aortic dissection
- A woman in her 20s with syncope
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/2/2026):
Today’s case by Drs. McArthur and McLaren serves to remind us of 2 important PEARLS in emergency medicine:
- #1) Although true Low Voltage on ECG is a relatively uncommon finding — it is associated with a number of important diagnostic considerations (shown below in Figure-1 — to which I’ve added today’s ECG).
- #2) Bedside Cardiac Echo is an amazing and invaluable tool that will occasionally solve what might otherwise be a problematic presentation — and — and it may do so in a matter of minutes. Among emergency conditions that come to mind for which bedside Echo may be lifesaving include: i) Detection of acute PE (Bedside Echo by a skilled operator greatly expedites diagnosis and treatment of potentially life-threatening PEs); — ii) Assessment of cardiac function (including detection of a localized wall motion abnormality that may expedite confirmation of acute OMI); — and, iii) Identification and relative quantification of pericardial effusion (and in today’s case — diagnosis of pericardial tamponade in need of urgent pericardiocentesis).
= = =
As per Drs. McArthur and McLaren — Today’s case is remarkable for the patient presenting with a blood pressure = 140/100 mmHg and without appearing ill or distressed despite having a large pericardial effusion complicated by signs of pericardial tamponade.
- Thepresenting ECG in Figure-1 is remarkable for sinus tachycardia, and especially for the generalized reduction in QRS amplitude, with multiple leads manifesting a QRS of ≤3 mm in size. This degree of low voltage should immediately prompt consideration of the causes listed in Figure-1 — for which bedside Echo in today’s case provided a quick, definitive answer.
- = = =
- NOTE: For easy reference — Our table of the Causes of Low Voltage can be easily found in the TOP Menu of every page in Dr. Smith’s ECG Blog.
= = =
Figure-1: I’ve reproduced today’s ECG — to which I’ve added our Table regarding the definition and important causes of Low Voltage. (Note: To improve visualization and adjust the ECG grid of today’s tracing — I’ve digitized the original ECG using PMcardio).

= = =
= = =