This was sent by Tom Fiero, from Merced CA, and an avid reader of the blog.
“A 41 yo man presented with sudden severe chest pain, onset 1 hour prior to arrival.”
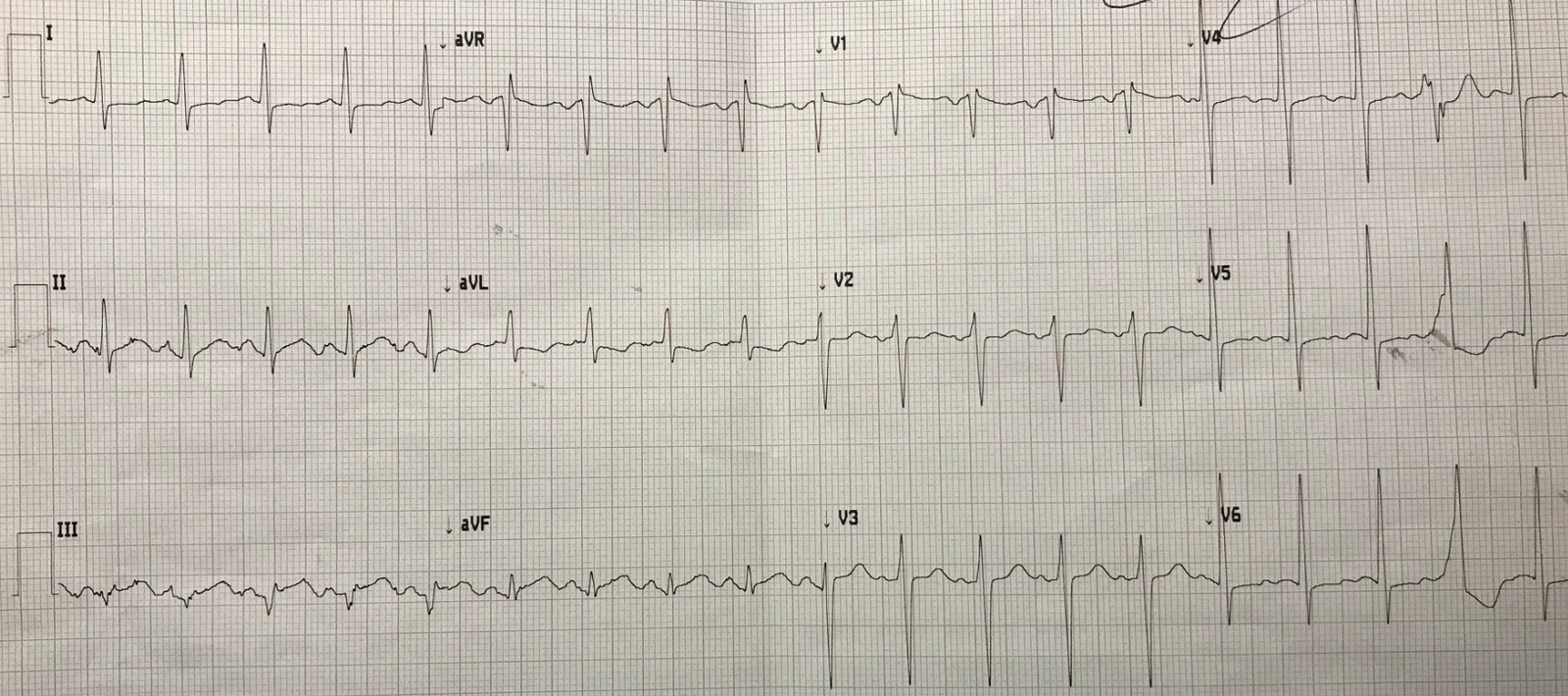
“Here is the first ED ECG at 2242:”
 |
| What do you think? |
“My partner was shown the ECG and he was not impressed.”
“30 minutes later, I picked up the patient and saw this ECG, and I was concerned.”
“I was worried about the slight ST depression in lead aVL, and the morphology of aVL.”
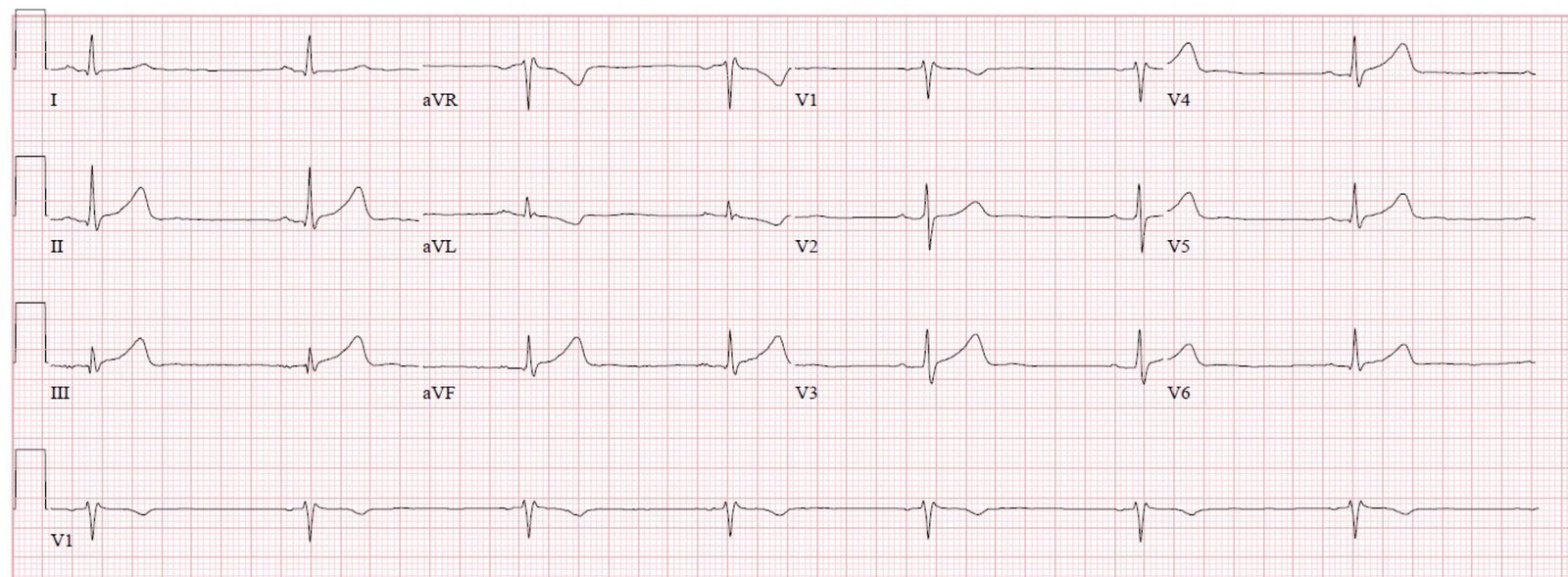
“I sought a previous ECG and found one from 9 months prior:”
 |
| Smith analysis:
Much different Old ECG: QRST axis = ~15 degrees Presentation ECG: QRST axis = ~ 0 degrees
So there really is no significant change in the QRST axis, which measures T-wave inversion, but there is a change in both the QRS axis and the T-wave axis, and I don’t really know the significance of this. Nevertheless, I agree with the reader that aVL looks suspicous, but not diagnostic. |
Dr. Fiero continues:
“At this point, the patient was also diaphoretic. I ordered aspirin and heparin bolus. BP was 220/110. I ordered sublingual NTG. I would order a NTG drip, but it holds up stat ground transfer because it requires a critical care nurse. So I ordered labetolol.”
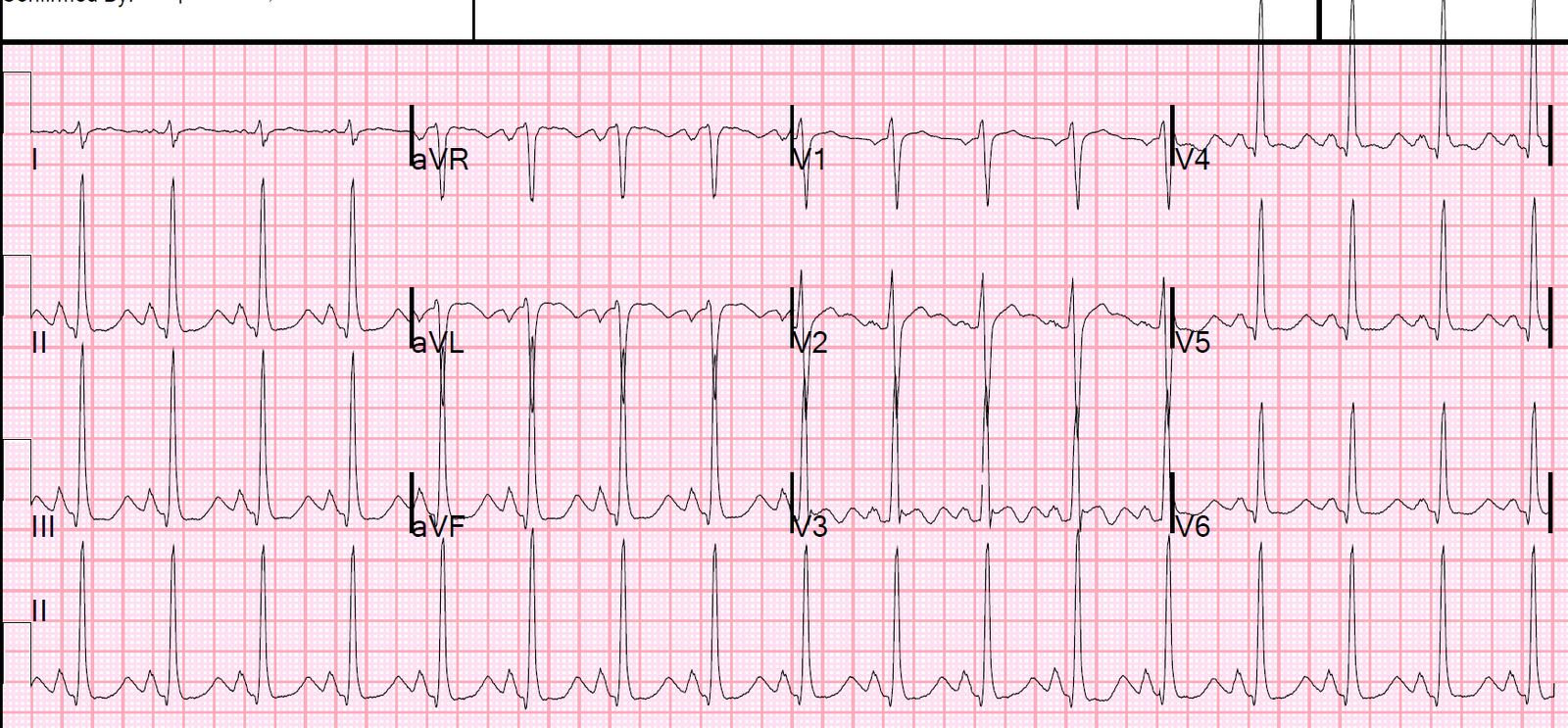
Then I ordered another ECG at 2316
 |
| “This is now obvious.”
Smith: Agree. Clearly an Inferior OMI |
“I ordered TNK-tPA (Tenectaplase), since the transport time is too long to rely on PCI alone.”
Smith comment:
1. If first medical contact to balloon time is greater than 120 minutes, which happens in more than 50% of transfers, then give thrombolytics and transfer for immediate PCI upon arrival.
Stated otherwise:
2. If door (at referring hospital) to balloon (at receiving center) time is greater than 90 minutes, then give thrombolytics. When transport time is greater than 30 minutes, door to balloon time is greater than 90 minutes in more than 50% of cases.
Fiero
“The patient was still having chest pain.”
“Door to needle is greater than 90 minutes, hence TNK.”
“And I recorded the 3rd ECG:”
2322
 |
| More obvious still |
“At this point, the patient was looking and feeling better. We loaded him up and sent him.”
“Before leaving, he admitted to amphetamine abuse about 10 hours prior to presentation.”
“I thought I was maybe over-reacting with first ECG.”
“Then I got the old EKG, and he looked ill, and I realized I was not overreacting.”
The patient reperfused his RCA and had a good outcome.
Smith comments
A couple further points on thrombolytics prior to transfer:
1. Clopidogrel is a good idea and proven beneficial when giving thrombolytics for STEMI. The dose in this situation is 300 mg.
—–Neither Prasugrel nor Ticagrelor have been studied, nor clopidogrel at a dose of 600 mg.
2. ASSENT-3 showed that the best antithrombotic for STEMI who are receiving thrombolytics is enoxaparin.
This is the dosing regimen
(all regimens must be agreed upon between the referral and receiving institutions):
STEMI with thrombolytics, even if followed by transfer with immediate PCI:
Enoxaparin is the optimal choice:
If less than 75 years old: 30 mg IV bolus, followed in 15 min by 1 mg/kg subQ (max 100 mg)
If over 75 years: No bolus, 0.75 mg/kg subQ (max 75 mg)
Transfer of patients with STEMI and
use of thrombolytics
Dr Meyers and I wrote the ACS chapter in the EmRap “CorePendium”
(Compendium of Emergency Medicine, an online Textbook). Here is the section on Transfer of
STEMI patients which I wrote.
Transfer for PCI-only vs. thrombolytics
prior to transfer for STEMI
- If
delay from first medical contact to PCI will be greater than 120 minutes
(and it almost always is) - Then
Thrombolytics first - If
delay is less than 120 minutes, then transfer for PCI without
thrombolytics
Facilitated PCI (thrombolytics) with
full adjunctive antithrombotic therapy and P2Y12 inhibition, when patient
cannot get PCI within one hour for STEMI
- STREAM
study (Armstrong et al.
2013). Patients presenting to non-PCI hospital.
All transferred. - Randomized to:
- 1) TNK-tPA before transfer
- Standard dose bolus
tenecteplase (½ dose in patients over 75 years of age) with clopidogrel
300 mg and enoxaparin (30 mg IV + 1 mg/kg subcutaneous) before transport
to a PCI-capable hospital. - 2) No TNK-tPA before
transfer - PCI-only group:
- Patients in the PCI-only
group were treated very fast, with 100 minutes from symptom onset
to sheath insertion (Armstrong et al. 2013) - Thrombolytic before PCI group:
- Emergency coronary
angiography was performed if fibrinolysis failed (this was measured by
resolution of pain and ST-segment elevation on the ECG). - Thus, it is analogous to
planned rescue PCI (see Rescue PCI below) - Otherwise, angiography was
performed 6 to 24 hours after randomization. - The primary endpoint was a composite of death, shock,
congestive heart failure, or reinfarction up to 30 days. - Results:
- 36% of lytic patients
required urgent PCI. Mean time from randomization to angiography
for these patients was 2.2 hours, vs. 17 hours for the other 64%. - The primary end point
occurred in 116 of 939 patients (12.4%) in the fibrinolysis group with
rescue, and in 135 of 943 patients (14.3%) in the primary PCI group
(p=0.21 - Intracranial hemorrhage was
1.0% for TNK-tPA vs. 0.2%. - Conclusion: Transfer for PCI without
thrombolytics is best if PCI at receiving facility can be done in less
than 120 minutes from first medical contact, or less than 90 minutes from
STEMI diagnosis in first ED.
Thrombolytics prior to Transfer to a
PCI capable facility, then rescue PCI if no reperfusion for STEMI
- TRANSFER AMI (Cantor
et al. 2009). - High
risk STEMI: BP less than 100, HR greater than 100 Killip class II, III, ST
depression of at least 2 mm in precordial leads, ST elevation in right
precordial leads (right ventricular MI - All
patients get TNK-tPA. - 80-90%
received clopidogrel 300 mg (75 mg for age over 75). - Enoxaparin
(not for age over 75) or UFH (50-50). Doses not specified,
presumably standard doses. - Patients
randomized to: - 1) Standard Rx:
- Transfer only if there is persistent ST
elevation (less than 50% ST resolution) - No transfer if there is reperfusion
(ST resolution) - 2) Transfer with immediate PCI regardless of
reperfusion. - Results: Intervention
group had PCI a median of 2.8 hours after randomization - 30-day severe adverse outcomes 17.2% vs.
11.0% (NNT = 16) - Conclusion: All high risk STEMI should be immediately transferred after
thrombolytics
Thrombolytics prior to transfer to a
PCI capable facility, then routine PCI regardless of reperfusion for
STEMI
- CARESS-in-AMI (Di Mario et al.
2008) - Patients: High risk STEMI, had at least one
high risk feature treated initially at non-PCI hospital - Extensive ST elevation, new LBBB, previous
MI, Killip class greater than or equal to 2, LVEF less than 35% - ½ dose reteplase, abciximab, heparin,
aspirin, only 1 in 6 received upstream clopidogrel, but this is probably
not so important because they did receive DAPT using abciximab. - Randomized to:
- Immediate transfer for PCI or
- Standard therapy: Transfer for rescue PCI
only if needed - PCI in 85.6% of immediate group; rescue PCI
in 30.3% of standard group - Median time from thrombolytics to transfer =
110 minutes in immediate group vs. 180 minutes in rescue group. - Composite of all-cause mortality,
reinfarction, and refractory myocardial ischemia within 30 days (4.4%
versus 10.7%, p = 0.004) in the immediate PCI group vs. standard
care/rescue PCI group (NNT=17). - No significant differences in major bleeding
at 30 days (3.4% versus 2.3%, P0.47) or stroke (0.7% versus 1.3%,
P0.50). - Meta-analysis
including both high risk and non-high risk patients - Concluded that all patients should be
transferred for early routine PCI after thrombolytics (Borgia et al. 2010). - Early was defined as less than 24 hours.
However, the figure below from an editorial (Granger 2011) representing the 7 trials
in the meta-analysis shows that the time to PCI was usually very short. - Conclusions:
- All high risk patients who receive
thrombolytics prior to transfer should have immediate angiography +/- PCI
at the receiving facility, regardless of reperfusion status (in other
words, not only the patients who need rescue PCI). - Among non high risk patients who do not need
rescue PCI, also consider immediate angio +/- PCI after a delay of 2-3
hours (O’Gara
et al. 2013).
Half dose thrombolytics prior to
transfer to a PCI capable facility for STEMI
- Half dose thrombolytics prior to transfer appears to be a
attractive option, without an increase in major bleeding. (Larson et al. 2012) - Not a randomized trial
- STEMI receiving center, with some referral
hospitals are more than 60 miles distant - Compared to STEMI patients presenting
directly to the receiving hospital - All received aspirin,
clopidogrel, and unfractionated heparin (UFH) - Those presenting to
hospitals ≥60 miles away also received half-dose fibrinolytic with
transfer for immediate PCI. - Total 2634 consecutive STEMI
patients from all sources - 660 transferred from remote
hospitals utilizing half-dose tenecteplase (TNK-tPA) - 600 patients who presented
directly to the PCI centre. - Door to balloon time for
direct vs. transfer: (mean +/- CI): 62 (44-83) vs. 122 (100-147) - No significant differences
in 30-day mortality (5.5 vs. 5.6%; P= 0.94), stroke (1.1 vs. 1.3%; P=
0.66), major bleeding (1.5 vs. 1.8%; P= 0.65), or
re-infarction/ischaemia (1.2 vs. 2.5%; P= 0.088) in patients receiving
TNK vs. those presenting directly to the PCI centre, despite a
significantly longer door-to-balloon time
Summary: Combination
Reperfusion Strategies (Thrombolytics + PCI)
- First,
it is important to realize that only a percentage of STEMI patients
who do not receive thrombolytics are actually transferred for PCI in a
timely fashion, and thus thrombolytics prior to transfer should be
strongly considered. - When drive time is over 30 minutes, only 42%
of patients achieve first door to balloon time in less than 120
minutes. Recommended time is first medical contact to balloon of time
of less than 120 minutes (Vora
et al. 2015). - Thus,
according to the ACC/AHA, immediate transfer after thrombolytics is
recommended: - For all failed reperfusion (for rescue PCI),
ST resolution at least 70% - For all high risk patients
- For all other patients, it is reasonable to
transfer - For these patients, PCI should be delayed
for 2-3 hours after thrombolytics (O’Gara
et al. 2013)
Finally,
Half dose thrombolytics prior to transfer appears to be a attractive option,
without an increase in major bleeding. (Larson et al. 2012)
![]()
===================================
MY Comment, by KEN GRAUER, MD (11/8/2019):
===================================
Interesting case by Drs. Tom Fiero and Stephen Smith, in which the title of this post tells all = “A 41yo with Chest Pain and Nondiagnostic Triage ECG”. My comments are focused on “Lessons Learned” from the first 3 tracings shown.
- For clarity — I’ve put these first 3 tracings shown together in Figure-1.
- Please NOTE: My Comments below are subtle and clearly advanced. Are you up for the challenge?
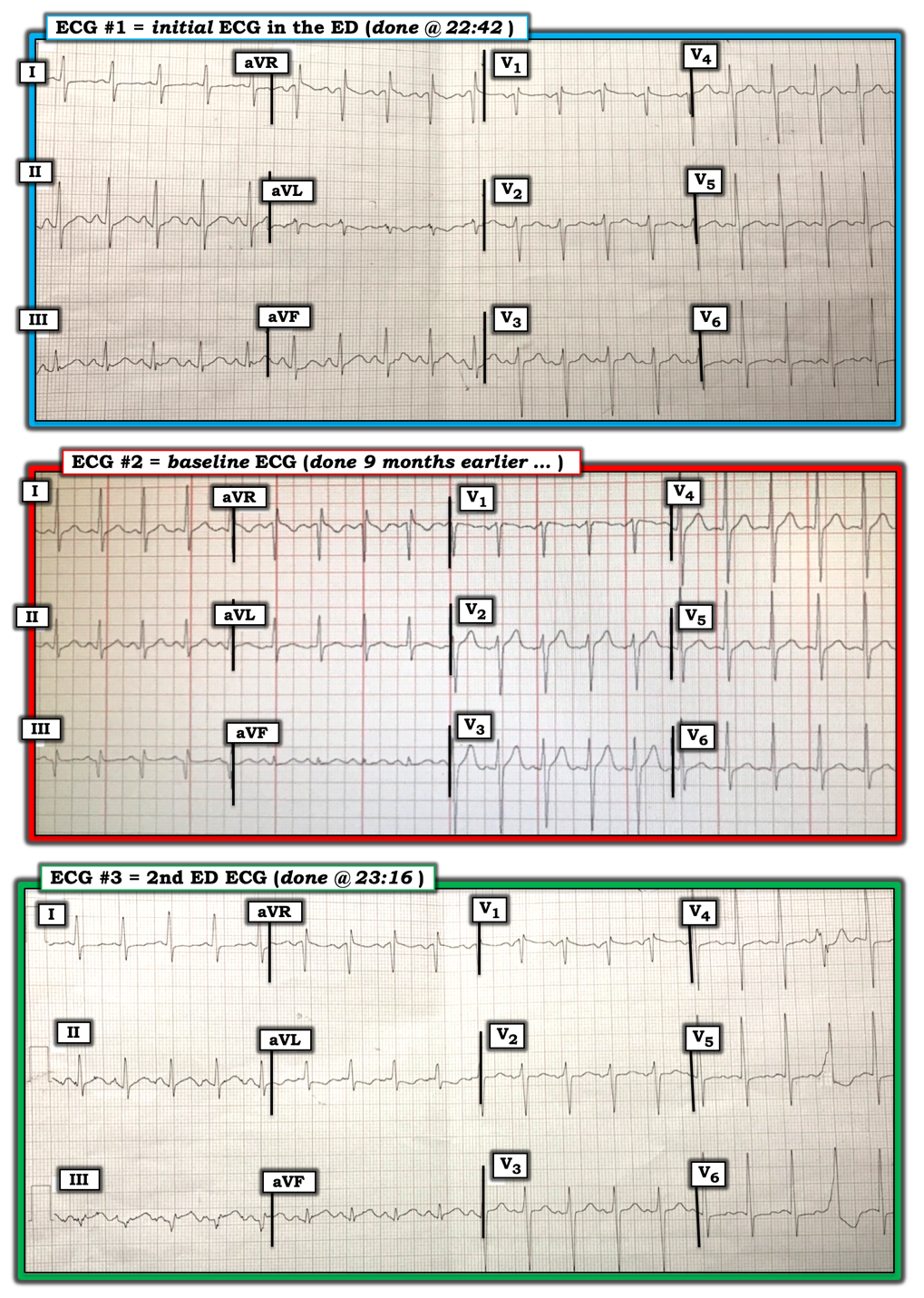 |
| Figure-1: The first 3 ECGs shown in this case (See text). |
ECG #1: As is often the case — the History is KEY.
- The patient is a 41yo man who presented with sudden severe chest pain that began 1 hour prior to arrival at the hospital. Given this worrisome clinical presentation — the onus of proof is on US to demonstrate that this is not OMI in progress, rather than the other way around …
Although ECG #1 is not diagnostic of acute OMI by itself — this is not a “normal” ECG.
- KEY Point: ECG #1 is not “negative” in the sense that it rules out anything. It is simply not diagnostic by itself of acute OMI.
- There is sinus tachycardia at 115-120/minute. As always with sinus tachycardia — we need to find out WHY?
- I suspect that lead V1 is placed too high on the chest because: i) there is a prominent negative component to the P wave in lead V1; ii) there is an r’ pattern in lead V1; and, iii) the overall appearance of lead V1 looks similar to that of lead aVR (CLICK HERE — for more on recognizing the likelihood of lead V1,V2 malposition).
- Otherwise for ECG #1 — The PR interval is normal, and the QRS is narrow. The QTc may be borderline — though it is difficult to know what to make of the QTc given the rapid rate. The frontal plane axis is normal (ie, around +75 degrees). There is no chamber enlargement. If lead V1 is not misplaced — then there is an incomplete RBBB pattern (ie, an r’ in V1 with narrow terminal s waves in leads I and V6). Regarding Q-R-S-T Changes — there are no Q waves (other than perhaps in lead V1) — and R wave progression shows slightly delayed transition (the R does not become taller than the S wave is deep until between leads V4-to-V5). There is persistence of S waves through to lead V6.
The most remarkable findings in ECG #1 are regarding ST-T Wave Changes. These need to be interpreted in light of the fact that this patient presented with new-onset and severe chest pain, that began just 1 hour before this tracing was done:
- There is non-specific ST-T wave flattening in a number of leads (ie, in leads I, V2, V5 and V6). The T wave is of relatively reduced amplitude in leads V3 and V4.
- There is T wave inversion in lead aVL of ECG #1. Although the T wave in lead aVL may normally be inverted when the QRS complex is predominantly negative in this lead — the size of this T wave (relative to the tiny size of the QRS in aVL) is disproportionately large and, this negative T wave in aVL looks fatter-than-it-should-be. This is a subtle change! That said, given the worrisome history — it should not be discounted!
- NOTE: Although there is no ST elevation in the inferior leads — Did YOU notice that ST-T wave morphology changes almost from beat-to-beat in each of the inferior leads in ECG #1? A few complexes in the inferior leads do manifest ST segment straightening — which could be an early sign of acute OMI if the T wave inversion in lead aVL was to reflect a “reciprocal” change. BUT — because of this changing ST-T wave morphology from beat-to-beat in the inferior leads, it is hard to know which ST-T waves reflect what is really happening … (This initial ED tracing should be repeated in short order).
BOTTOM Line Interpretation of ECG #1: Although ECG #1 is non-diagnostic of acute OMI — this is not a normal tracing. By itself it rules nothing out. BUT:
- More information is needed before any conclusions can be reached. This includes repeating the ECG in short order (ideally within a few minutes) — looking for prior tracings on this patient — stat Echo at the bedside (looking for wall motion abnormality) — serial troponins — and, continued close observation of the patient until there can be greater certainty about the diagnosis.
QUESTION: A baseline tracing (done 9 months earlier) was found ( = ECG #2). What differences do you see between ECG #1 and ECG #2? Does finding this previous ECG change your assessment of what you saw in ECG #1?
- HINT: Be sure to do a lead-by-lead comparison of these 2 tracings in Figure-1.
ANSWER:
- ECG #2 — again shows sinus tachycardia at a similar rate! This again raises the question of WHY is there sinus tachycardia? NOTE: This is relevant to this case — since much of the value of a comparison tracing might be lost IF the patient presented with similar circumstances (ie, new-onset chest pain) 9 months earlier when the previous ECG ( = ECG #2) was done.
- As noted by Dr. Smith — there is no T wave inversion in lead aVL of ECG #2 — BUT — the frontal plane axis is quite different! That is, the QRS complex in both leads I and aVL of ECG #2 is now clearly positive. Thus, although the relative size and shape of the T wave inversion in ECG #1 should still raise suspicion of an acute change — the shift in frontal plane axis between the 2 tracings negates making any definitive conclusion.
- There is a wide and deep Q wave in lead III of the baseline tracing ( = ECG #2). This is not seen in ECG #1. The significance of this finding is uncertain.
- There has been a change in ST-T wave morphology between the 2 tracings in multiple leads! That is, the ST-T wave was upright and of normal appearance in leads I, V2, V3, V4 and V5 in the baseline tracing ( = ECG #2). And, even though the T wave was smaller-than-it-should-be in leads aVL and V6 of ECG #2 — the ST-T wave in these leads clearly looks more abnormal in ECG #1.
BOTTOM Line Comparison Assessment: Both tracings show sinus tachycardia at a similar rate. BUT — at least 7 leads show an increase in nonspecific ST–T wave changes on the new tracing ( = ECG #1).
- Once again — More information is needed before any conclusions can be reached. Nevertheless, given the worrisome history and, this patient’s worsening appearance (ie, as noted by Dr. Fiero above, the patient was now diaphoretic) — even though ECG #1 remains non-diagnostic — a high index of suspicion needs to be maintained!
A 2nd ECG in the ED ( = ECG #3 in Figure-1) was done at 23:16 ( = 34 minutes after ECG #1). While now obvious that ECG #3 confirms the diagnosis of acute OMI — I think it helpful to describe: i) the lead-by-lead changes that have occurred in the 34 minutes between ECG #1 and ECG #3 (Figure-1); and, ii) to take another look at the baseline ECG ( = ECG #2) in the interest of now determining with more certainty which changes in ECG #1 were indicative of this acute evolving event.
- ECG #3 — again shows sinus tachycardia at a similar rate. There is a PVC.
- There is now hyperacute ST elevation in leads III and aVF (and probably also in lead II ) of ECG #3.
- NOTE: The frontal plane axis in ECG #3 is now similar to what it was in the baseline ECG ( = ECG #2) — BUT — despite a predominantly positive QRS complex in lead aVL of ECG #3 — the T wave is inverted, in association with slight-but-real J-point ST depression in this lead! This mirror-image opposite ST-T wave picture in leads III and aVL of ECG #3 confirms the diagnosis of acute inferior OMI in this patient with new severe chest pain. It also confirms (albeit in retrospect) — that the suspicious shape of the T wave inversion in lead aVL of ECG #1 was in fact, a sentinel ST–T wave change warning of imminent acute inferior OMI, even though ECG #1 was not yet diagnostic at that point (since inferior lead hyperacute ST elevation had not yet begun).
- Assessment of all 3 tracings in Figure-1 also allows us (again, albeit in retrospect) — to conclude that the increase in nonspecific ST-T wave changes in at least 7 leads in ECG #1 compared to baseline ECG #2 was also indication of this patient’s imminent infarction.
Our THANKS to Drs. Fiero and Smith for presenting this case. CREDIT to Dr. Fiero — for excellent management of this case!
![]()
–>