===================================
MY Comment by KEN GRAUER, MD (3/12/2020):
===================================
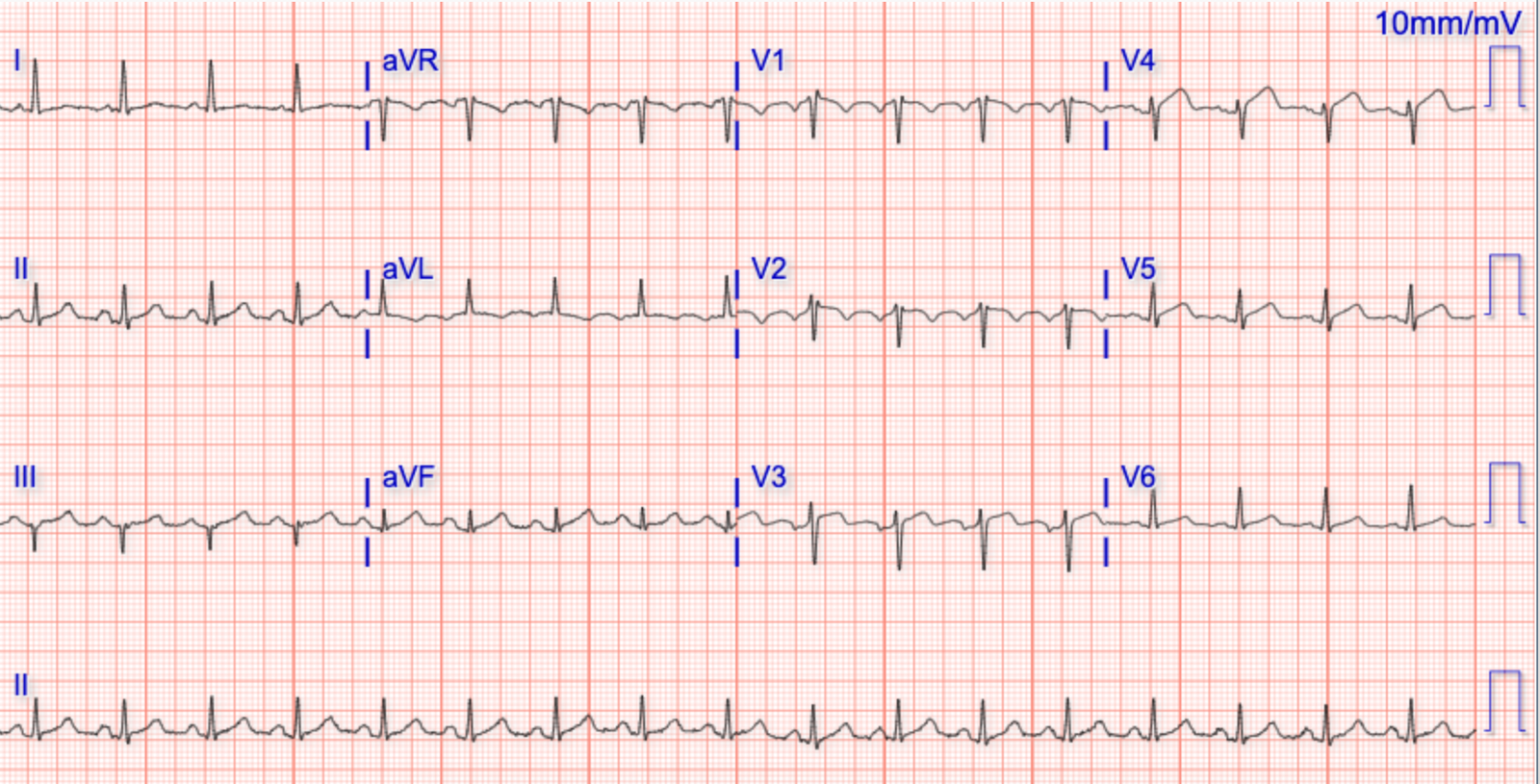
A young adult presented to the ED with the “heart awareness” and the ECG shown in Figure-1 — but with no more than slight shortness of breath. BP ~ 130/70.
QUESTIONS:
- What is the cardiac rhythm?
- How certain are you of your diagnosis?
- Is the clinical scenario consistent with what you might expect for this rhythm?
 |
| Figure-1: The initial ECG in the ED (See text). |
ANSWERS: This young adult appears to be hemodynamically stable — since his BP is normal and his symptoms are minimal. Knowing this gives us time to focus on the cardiac rhythm. As emphasized in previous posts — I favor a Systematic Approach for the interpretation of any cardiac rhythm, based on assessment of 5 Parameters. These 5 parameters are easily remembered by the saying, “Watch your Ps, Qs & the 3 Rs” (See My Comment in the October 16, 2019 post).
- The rhythm in Figure-1 is fast, and irregularly irregular. Although there are some undulations (small deflections) in the baseline (particularly in leads III and V1) — there is no clear sign of P waves. The QRS complex is obviously wide. Putting these ECG findings together — you have described an irregularly irregular WCT ( = Wide-Complex Tachycardia) without clear sign of P waves in any of the 12 leads.
- NOTE: On occasion — VT (Ventricular Tachycardia) can be slightly irregular. That said — it is highly unlikely for VT to manifest the degree of irregular irregularity from one beat-to-the-next that we see in ECG #1. Therefore — the rhythm in ECG #1 is almost certain to be AFib (Atrial Fibrillation), seen here with a “rapid” ventricular response.
- CLICK HERE — for more on the ECG diagnosis of irregular WCT rhythms.
QUESTION:
- HOW FAST does the rhythm in ECG #1 get in some parts of the tracing? (Please see Figure-2 when addressing this question, in which I have numbered the beats in the initial ECG).
 |
| Figure-2: The beats in ECG #1 have been numbered (See text). |
ANSWER: As noted above — the rhythm in ECG #1 is irregularly irregular. The shortest R-R intervals in this tracing are barely more than 1 large box in duration (ie, seen for the R-R intervals between beats #5-6; 10-11; 20-21; 26-27; and 30-31). This short R-R interval duration corresponds to a ventricular response that at times attains a rate of between ~220-250/minute!
- Under normal conditions with AFib — the refractory period of the AV node does not allow more than 150-to-200 impulses/minute to be conducted to the ventricles. A ventricular response that at times attains a rate of ~220-250/minute is simply too fast for atrial impulses to be transmitted over the normal (AV nodal) conduction pathway.
- PEARL #1: Recognition that AFib with a wide QRS complex attains a ventricular response that at times exceeds 220/minute — instantly tells you that the patient must have WPW (Wolff-Parkinson-White) Syndrome, in which AFib impulses are by-passing the AV node, and are being conducted to the ventricles over an AP (Accessory Pathway).
- PEARL #2: In addition to an excessively rapid ventricular response — another characteristic ECG finding of AFib in a patient with WPW is a surprisingly large variation in R-R intervals, in which some of the longer R-R intervals are more than twice as long as the shortest R-R intervals (ie, as occurs for the R-R intervals between beats #7-8; and 21-22).
- PEARL #3: Surprisingly, these younger adult patients with WPW who develop very rapid AFib will often remain hemodynamically stable for long periods of time despite the exceedingly rapid ventricular response (similar to the very rapid rate seen in ECG #1) that may develop. This is another “soft” clue that the rhythm is not VT, in which the patient is likely to be more symptomatic.
- CLICK HERE and HERE — for more on the ECG diagnosis of arrhythmias in patients with WPW.
- PEARL #4: Not all patients with WPW are at risk of developing potentially life-threatening tachyarrhythmias. The risk of developing VFib during AFib in a patient with WPW is greatly increased when the SPERRI (Shortest Pre-Excited R–R Interval) measures below 220-250 msec. This corresponds to a shortest R-R interval that is barely more than one large box in duration — which is essentially what we see for the R-R intervals between beats #5-6; 10-11; 20-21; 26-27; and 30-31 in ECG #1. Given this high risk of developing a potentially lethal WPW-associated arrhythmia — the young adult patient in this case would be best advised to strongly consider undergoing catheter ablation of his AP. (CLICK HERE — for more on risk assessment of the patient with WPW).
FOLLOW-UP: The patient in this case was electrically cardioverted. The resultant rhythm is shown in ECG #2 (See Figure-3).
 |
| Figure-3: The post-cardioversion tracing is shown below the initial ECG (See text). |
QUESTION:
- Does the post-cardioversion tracing in Figure-3 support or go against the diagnosis of very rapid AFib that we saw for the rhythm in Figure-1?
ANSWER: Sinus rhythm has been restored in ECG #2. Note that the QRS complex in this post-cardioversion tracing is wide — and the PR interval is very short. A positive or negative delta wave is seen in virtually every lead. This confirms that this patient has WPW.
- Careful comparison of QRS complexes in each of the 12 leads in ECG #1 and ECG #2 reveals a very similar QRS morphology in the 2 tracings. This strongly supports our conclusion that ECG #1 indeed represented very rapid AFib in this patient who we have confirmed to have WPW.
======================
Acknowledgment: My sincere THANKS to Otis Rush (of Australia) for sharing the tracings and this case with us!
![]()
Smith comment:
There is one thing that Ken did not mention that makes this an obvious case of atrial fib with WPW: The polymorphic QRS complexes.
DDx of Polymorphic wide tachycardia:
1. polymorphic VT or
2. atrial fib with WPW.
DDx of irregularly irregular wide complex tachycardia:
1. polymorphic VT or
2. atrial fib with WPW.
3. Atrial fib with aberrancy or bundle branch block
4. Multifocal Atrial Tachycardia (MAT) with aberrancy or bundle branch block
Let’s go through this differential
–This is clearly NOT polymorphic VT.
–It is clearly not MAT.
–It is the polymorphic QRS that make it clearly WPW, in addition to the presence of RR intervals that are extremely short (as Ken mentioned).
Atrial fib with WPW always has these features:
1. Wide complex tachycardia
2. Irregularly irregular
3. Polymorphic QRS complexes.
People often ask me how you differentiate atrial fibrillation with aberrancy (say RBBB, or LBBB) from atrial fib with WPW.
Answer: Every QRS looks the same with BBB. In WPW, they do NOT all look the same.