This patient complained of prolonged vomiting and abdominal pain.
 |
| With this history, the ECG is pathognomonic. What is it? |
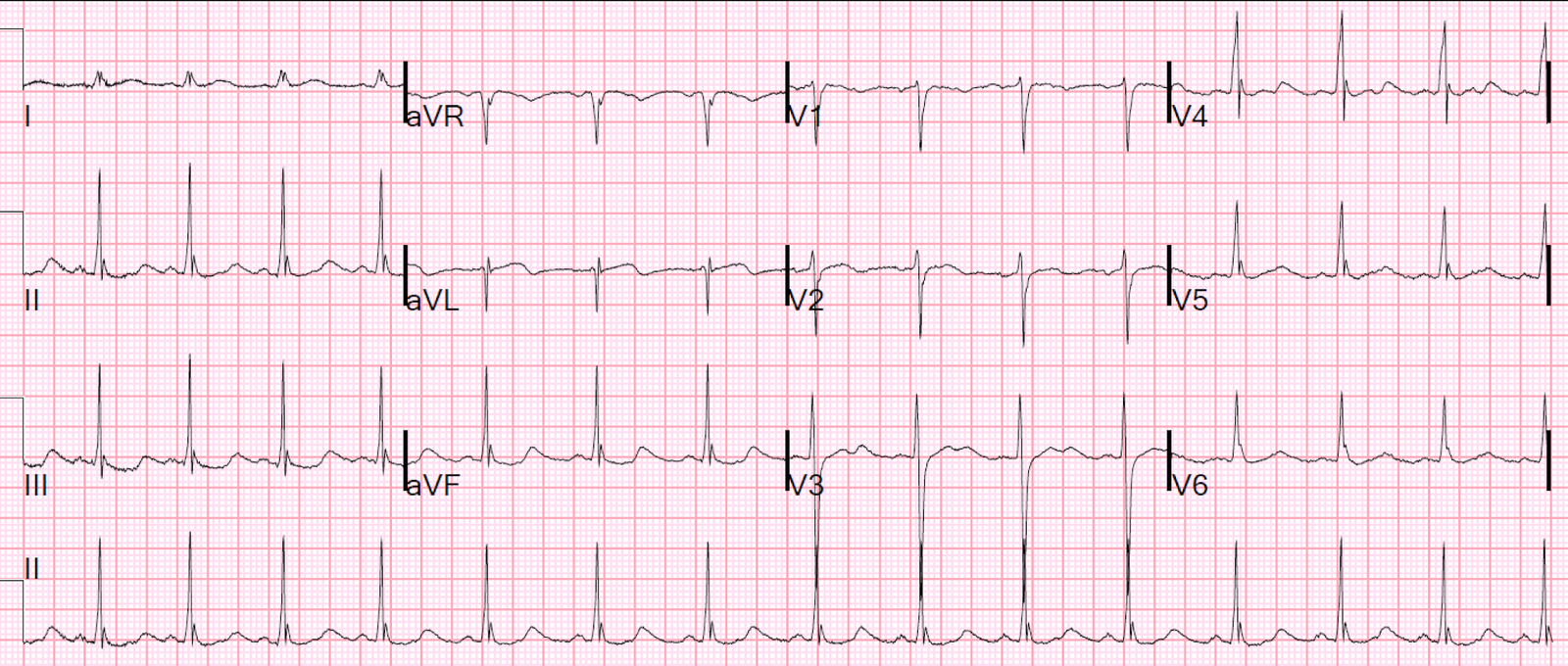
First, there are narrow J-waves that are similar to Osborn waves. The temperature was normal. I am not certain, but I believe these are just exaggerated J-waves with nonspecific etiology.
More importantly, there are large U-waves best seen in leads V3 and V4. You can also see that lead II has no visible T-wave but only a large U-wave. (If you look at V3 directly above lead II, you see both a T-wave and U-wave. If you follow that down to lead II below, you see no T-wave corresponding to the T-wave in V3, only a large U-wave. This is also true for V5 and V6.) Thus, what appears to be a long QT interval in these leads is really the QU interval.
This is nearly pathognomonic for hypokalemia. The K was 2.4 mEq/L. Magnesium was normal.