One of my residents who is very smart sent me this ECG.
Patient had “nonspecific chest symptoms worried she had pneumonia. She does not have pneumonia.”
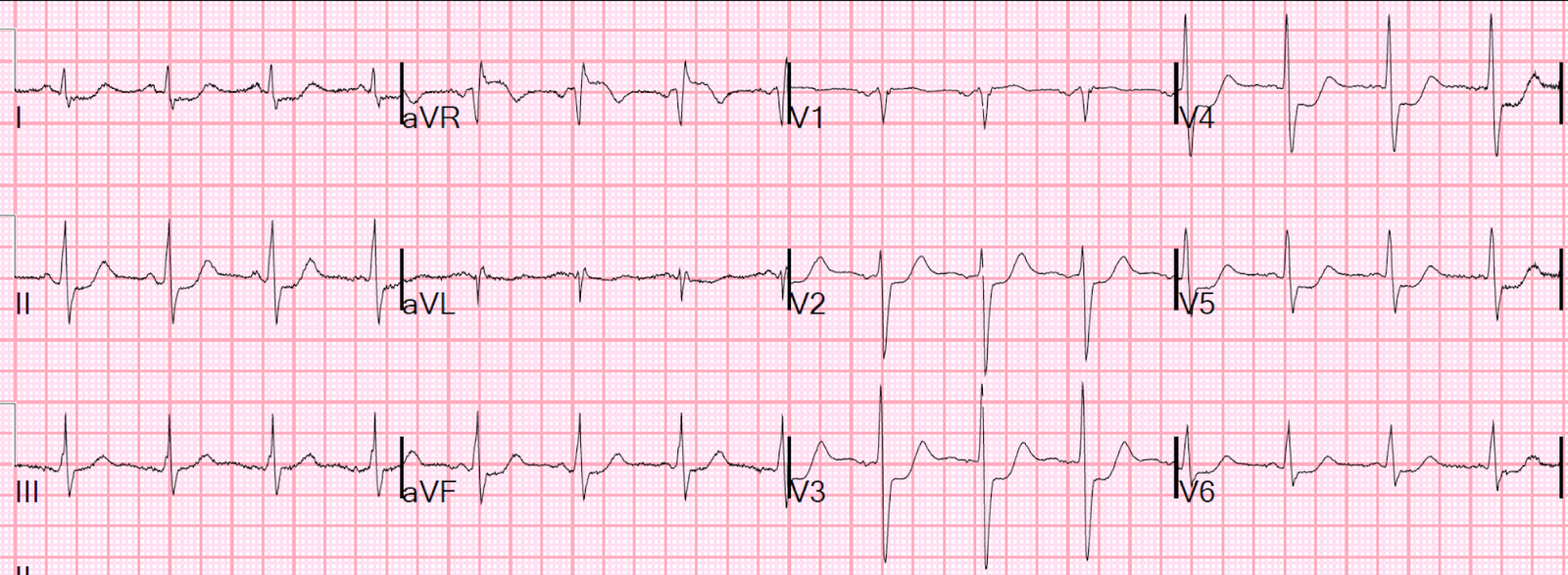
Here is the ECG:
 |
| What do you think? The resident wrote: She has 3 different QRS morphologies:, 1. One that looks narrow 2. One that looks LBBB 3. One that looks RBBB. Cardiology called them PVCs in their note, and I think the RBBB looking morphologies are PVCs with compensatory pause, but the LBBB ones clearly are not. |
Here is my interpretation:
At a
normal heart rate, the patient has left bundle branch block. But this
left bundle has a long refractory period. Thus, whenever the next beat
comes less shortly after the previous one, there is left bundle
branch block. Whenever the next beat comes later after
the previous, there is normal conduction.
That’s where the PVC is coming to
play: every PVC is followed by a compensatory pause that is long, which
gives the left bundle the time to repolarize.
The PVC comes from the LV and has RBBB morphology.
The LBBB comes from a long refractory period during normal sinus rhythm at a rate of 75 (RR interval 800 ms, less than 1 sec)
The normal conduction comes after a long RR interval caused by the compensatory pause (longer than 1 second).
![]()
===================================
MY Comment by KEN GRAUER, MD (4/22/2020):
===================================
— An interesting example of Rate-Related BBB:
I LOVE this case by Dr. Smith — because it highlights an important (albeit not overly common) phenomenon that can prove invaluable for explaining why a series of wide beats are not of ventricular etiology. The patient in this case study presented to the ED with the 12-lead tracing shown in Figure-1:
- The only clinical information we are provided with is that this patient had “nonspecific chest symptoms” that she thought was due to pneumonia. But she did not have pneumonia … And we don’t know the age of the patient (which would be relevant for predicting likelihood of underlying heart disease).
 |
| Figure-1: The initial ECG in this case (See text). |
As per Dr. Smith — the KEY to determining the etiology of the 3 different QRS morphologies that we see in ECG #1 lies with the R-R intervals preceding each of the beats in this tracing.
- I focus My Comment on some additional aspects of this case that I found interesting.
QUESTIONS:
- Is there LBBB (Left Bundle Branch Block) in Figure-1?
- If so — WHAT are the clinical implications of diagnosis of this form of conduction block?
- EXTRA Credit Questions: Do regular sinus P waves continue throughout the entire tracing? (ie, HOW MANY sinus P waves are there in the long lead II rhythm strip?). And — How does the answer to this question help in confirming the etiology of beats #3, 9 and 11?
MY THOUGHTS on ECG #1: Focusing first on the long lead II rhythm strip at the bottom of this tracing — the underlying rhythm in Figure-1 is sinus at a rate of ~70/minute. There is actually slight variation in the P-P interval in this tracing — though not enough (ie, not ≥0.12 second) to qualify as sinus “arrhythmia”.
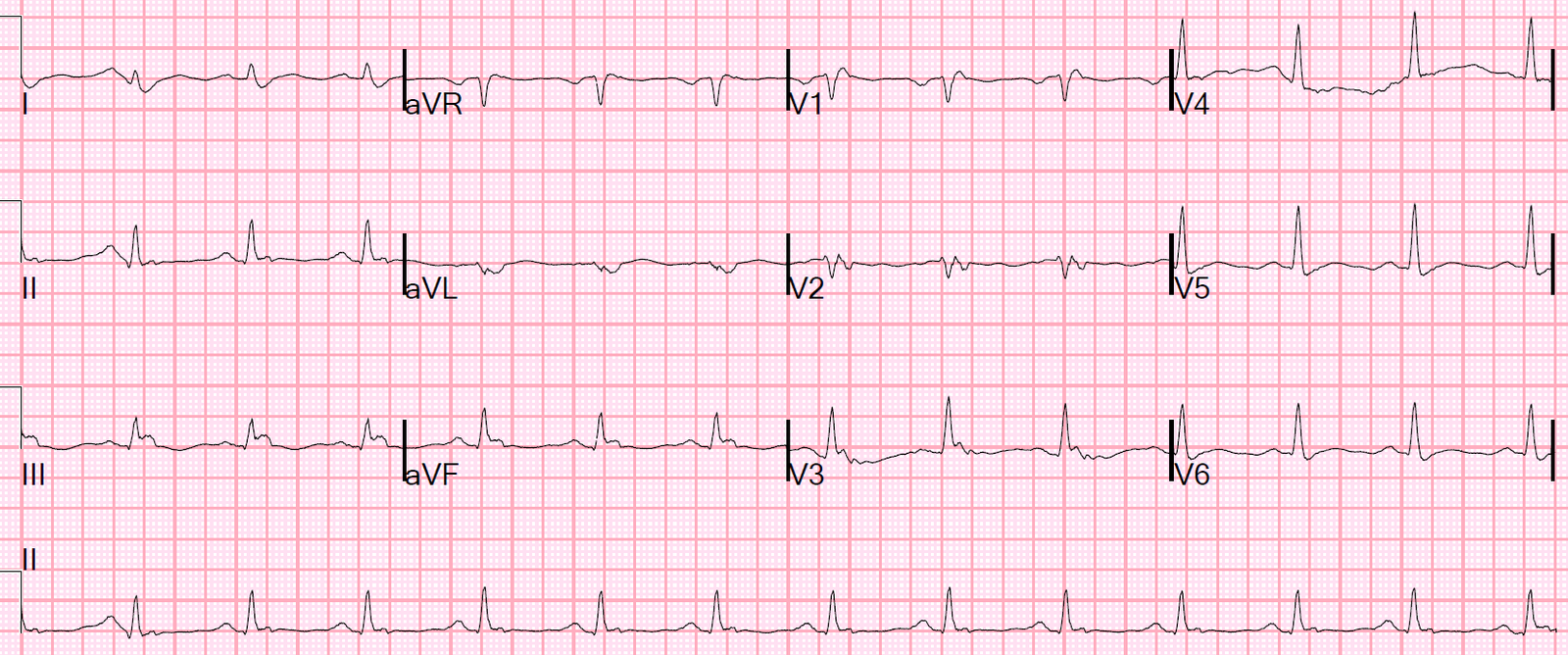
- I’ve labeled sinus P waves in Figure-2. RED arrows indicate obvious sinus P waves — that are upright with a constant PR interval in lead II. The other-colored arrows represent sinus P waves that aren’t so obvious.
- I’ve added PINK arrows to the long lead II rhythm strip to indicate sinus P waves that notch (distort) the T waves of beats #1, 3, 9 and 11. The reason we know these PINK arrows indicate the occurrence of on-time sinus P waves — is that even though partially hidden by the T waves of beats #1, 3, 9 and 11 — i) Calipers tell us that ongoing sinus P waves should be occurring at precisely the place where I’ve added the PINK arrows; ii) there is a prominent notch that peaks the first 2 of these T waves — with a slightly different (ie, rounder) appearance at the peak of the T waves for beats #9 and 11 (exactly as you’d expect with slight variation in the sinus P-P interval, as we see here); and, iii) PURPLE arrows in selected simultaneously-recorded leads more distinctly show the “telltale notching” of partially-hidden P waves within the T waves of beats #3, 9 and 11.
- PEARL #1: The reason why it is clinically useful to establish that sinus P waves continue throughout the entire long lead II rhythm strip (ie, there is a total of 12 sinus P waves in this rhythm strip) — is that this finding confirms that beats #1, 3, 9 and 11 must be of ventricular etiology. That is, since the underlying sinus rhythm is undisturbed thoughout the long lead II rhythm strip — the only plausible explanation for how beats #3, 9 and 11 could occur early — is that these beats must be arising from “below” (ie, from the ventricles). They can’t be aberrantly conducted PACs or PJCs — because both of these types of premature beats would have “reset” the sinus cycle!
- NOTE: Clearly, we already knew from ECG #1 that beats #1, 3, 9 and 11 are of ventricular etiology — because these beats are wide, they are not preceded by an early P wave, and their QRS complex looks very different than the normally conducted (ie, narrow) sinus beats #2, 4, 10 and 12. My point in presenting Pearl #1 — is that sometimes you will not be able to be certain about the etiology of an early wide beat — and recognition (by use of calipers) that the underlying sinus rhythm continues in its regular cadence despite the early wide beat will confirm that the wide beat is ventricular in etiology.
 |
| Figure-2: I’ve labeled sinus P waves in a number of leads. Note from the RED and PINK arrows in the long lead II rhythm strip that regular sinus P waves continue throughout the entire tracing (See text). |
From WHERE in the Ventricles Do Beats #1, 3, 9 and 11 Arise?
While fully acknowledging that the answer to this question is not important clinically — in the interest of “honing” your ECG interpretation skills — I think it educational to point out the following:
- That there is a very typical RBBB morphology to beats #1, 3, 9 and 11 — in the form of a QR pattern in lead V1 (and an rR’ in V2, and an rSr’ in V3) — that occurs in association with a fairly narrow initial R wave with wide terminal S wave in lateral leads I and V6.
- QRS duration of these wide beats is not overly long (I estimate ~0.12 second).
- QRS morphology of beat #3 in leads II and III is perfectly consistent with a LAHB pattern.
- BOTTOM Line: The finding of early beats that we know are ventricular in etiology — which manifest a highly typical RBBB/LAHB morphology, but which are not overly wide — suggests that beats #1, 3, 9 and 11 are probably “fascicular beats” arising from the left posterior hemifascicle. NOTE: Clinical implications of fascicular beats are the same as PVCs — so distinction between these 2 forms of premature ventricular complexes won’t alter initial management. But the concept of using all 12 leads on the ECG to assess QRS morphology is a useful one.
What about LBBB Conduction?
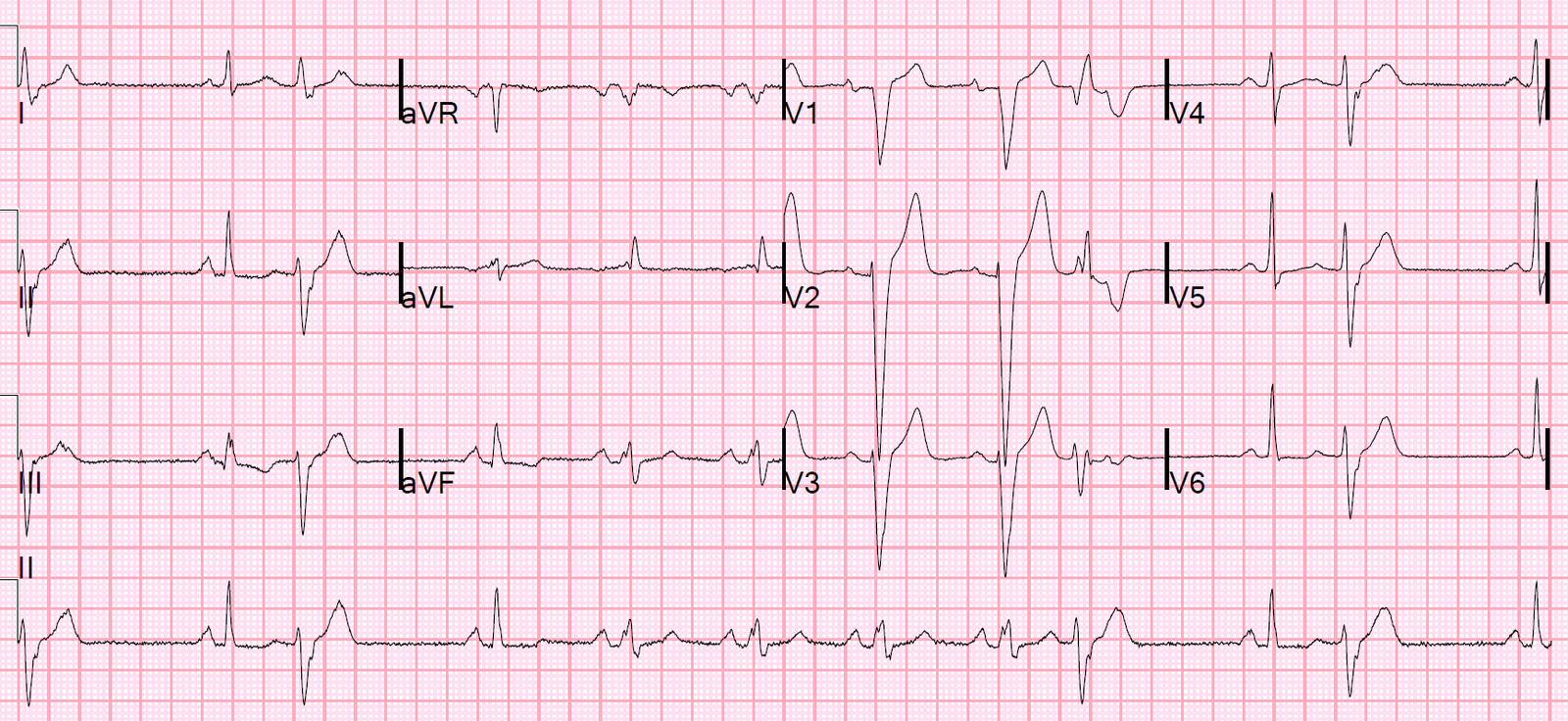
As per Dr. Smith — the reason beats #2, 4, 10 and 12 are conducted normally (ie, with a narrow QRS complex) — whereas sinus-conducted beats #5, 6, 7 and 8 are conducted with a wide QRS complex — is that the R-R interval preceding these wide, sinus-conducted beats is less than the R-R interval preceding the narrow sinus-conducted beats #2, 4, 10 and 12 (Figure-3):
- QRS morphology of the sinus-conducted wide beats (ie, beats #5, 6, 7 and 8) is consistent with LBBB conduction. This is easiest to appreciate in simultaneously-recorded leads V1, V2 and V3 — which are predominantly negative (with a straight and very steep S wave descent), as is highly characteristic of LBBB conduction. NOTE: Although the QRS complex of beats #5 and 6 in lead aVL looks deceptively narrow — this is because the initial portion of the QRS complex for beats #5 and 6 in lead aVL lies on the baseline (See vertical BLUE line in leads aVR, aVL and aVF that begins at the onset of the QRS complex). Therefore, there is an all positive QRS complex in lead aVL for the wide, sinus-conducted beats as expected with LBBB conduction (albeit part of the QRS in lead aVL is flat and lies on the baseline).
- The phenomenon of intermittent bundle branch block conduction during periods when heart rate increases is known as a rate–related BBB. While true that the longer R-R interval preceding beat #4 prolongs the subsequent Relative Refractory Period (via the Ashman phenomenon) — I would have expected even a prolonged RRP to have finished by 860 msec. (ie, It is when BBB or hemiblock conduction is seen following a short preceding R-R interval that we say there is aberrant conduction).
 |
| Figure-3: I’ve added measurements of the R-R interval preceding narrow beats #4, 10 and 12 — and preceding wide beats #5, 6, 7 and 8 (in milliseconds). The heart rate that these R-R intervals correspond to appears in parentheses (See text). |
PEARL #2: The phenomenon of a true rate-related BBB is not common in my experience. It is often quite challenging to recognize. The reason for the elusiveness of this dagnosis — is that most of the time, the QRS complex in patients with intermittent, rate-related BBB will be narrow — and, the parameters under which intermittent BBB is seen may change.
- KEY Point: The rate of onset of BBB conduction is often not the same as the rate where normal conduction resumes. For example — in Figure-3 — we see onset of LBBB conduction with beat #5 (preceding R-R interval = 860 msec, corresponding to a heart rate ~70/minute). Assuming 70 beats/minute as the rate of “onset” of rate-related BBB conduction — the heart rate may need to decrease to well under 70/minute before rate-related BBB resolves (perhaps to 60/minute or even slower). Therefore, rate of onset of rate-related BBB is not necessarily equal to the rate of offset for this conduction defect! Further complicating recognition of this phenomenon is the clinical reality that other conditions (ie, ischemia, hypoxemia, electrolyte imbalance, etc.) may all contribute to alter the onset/offset rate parameters.
- NOTE: I have not conclusively proven that there is rate-related BBB in Figure-3. That’s just my suspicion. We have not been provided with a baseline tracing in which there are no PVCs (and no abrupt changes in heart rate). We have also not been given other tracings that show normal (narrow) conduction with slower heart rates — in which non-PVC-related sinus acceleration results in BBB conduction. In my experience — it often takes extended follow-up of a given patient over time to prove that the reason for QRS widening is true rate-related BBB.
- CLINICALLY — Awareness that a given patient manifests intermittent rate-related BBB is most helpful when the underlying rhythm is AFib — because there are no “tell-tale” P waves in this case — and it could be easy to mistake rate-related BBB for a slightly irregular VT (CLICK HERE for an example of this).
PEARL #3: The clinical implications of an intermittent, rate-related BBB are similar to clinical implications of permanent BBB.
- In general — the significance of any conduction defect depends on the clinical setting in which it occurs. While incidental discovery of a longterm, bifascicular block such as RBBB/LAHB in an asymptomatic elderly patient clearly suggests the presence of some underlying heart disease — the risk of needing a permanent pacemaker is not necessarily that great. In contrast — new occurrence of RBBB/LAHB in a patient with acute proximal LAD occlusion poses a much greater risk of needing emergency pacing.
- In this case — we know neither the age of the patient, nor the past medical history. But, in contrast to complete RBBB (which sometimes is seen in patients without underlying heart disease) — LBBB (be it permanent or intermittent and rate-related) virtually never occurs in the absence of some form of underlying heart disease.
- PEARL #4: Determination of LVH on ECG is clearly more difficult in the presence of LBBB — because this conduction defect completely alters the sequence of ventricular depolarization and repolarization. As a result — the “usual criteria” for ECG diagnosis of LVH when the QRS is narrow are not valid with LBBB. That said, the presence of a very deep S wave in one or more of the anterior leads (ie, ≥25-30 mm) in a patient with LBBB — strongly suggests there is LVH (Note the S wave in lead V2 of ECG #1 is 32 mm!). Recognizing the patient in this case also has LVH is yet another indicator of underlying heart disease.
P.S.: Now that we have finally identified the etiology for each of the 3 different QRS morphologies in this tracing — we can turn our attention to assessment of atrial abnormalities and ST-T wave changes:
- The tall (ie, ≥2.5 mm) pointed P wave for sinus beats in the long lead II rhythm strip suggests RAA (Right Atrial Abnormality).
- To assess ST-T wave abnormalities — I focus on those sinus-conducted beats with a narrow (ie, normal) QRS complex. This includes beat #2 (in leads I, II, III) — beat #4 (in leads aVR, aVL, aVF) — and beats # 10 and 12 (in leads V4, V5, V6). Looking at these beats — I see nonspecific ST-T wave flattening, with some slight depression in the infero-lateral leads — but no acute changes.
Our THANKS to Dr. Smith for presenting this interesting case.
![]()