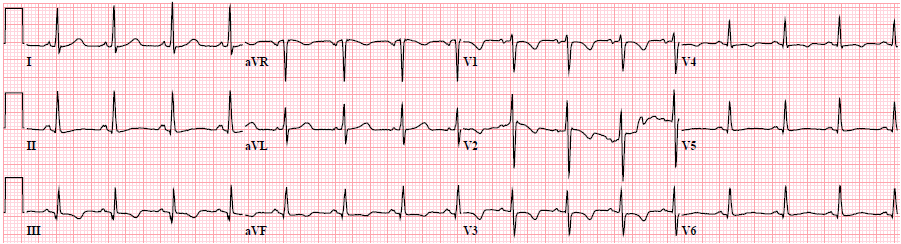
A young woman had what sounded like vasovagal syncope. This ECG was recorded:
 |
| There is incomplete RBBB (QRS = 110 ms). There is some ST depression and T-wave inversion in V1-V3, but remember this is the normal repolarization pattern for RBBB. What else? |
It looks like a very long QT.
Is it?
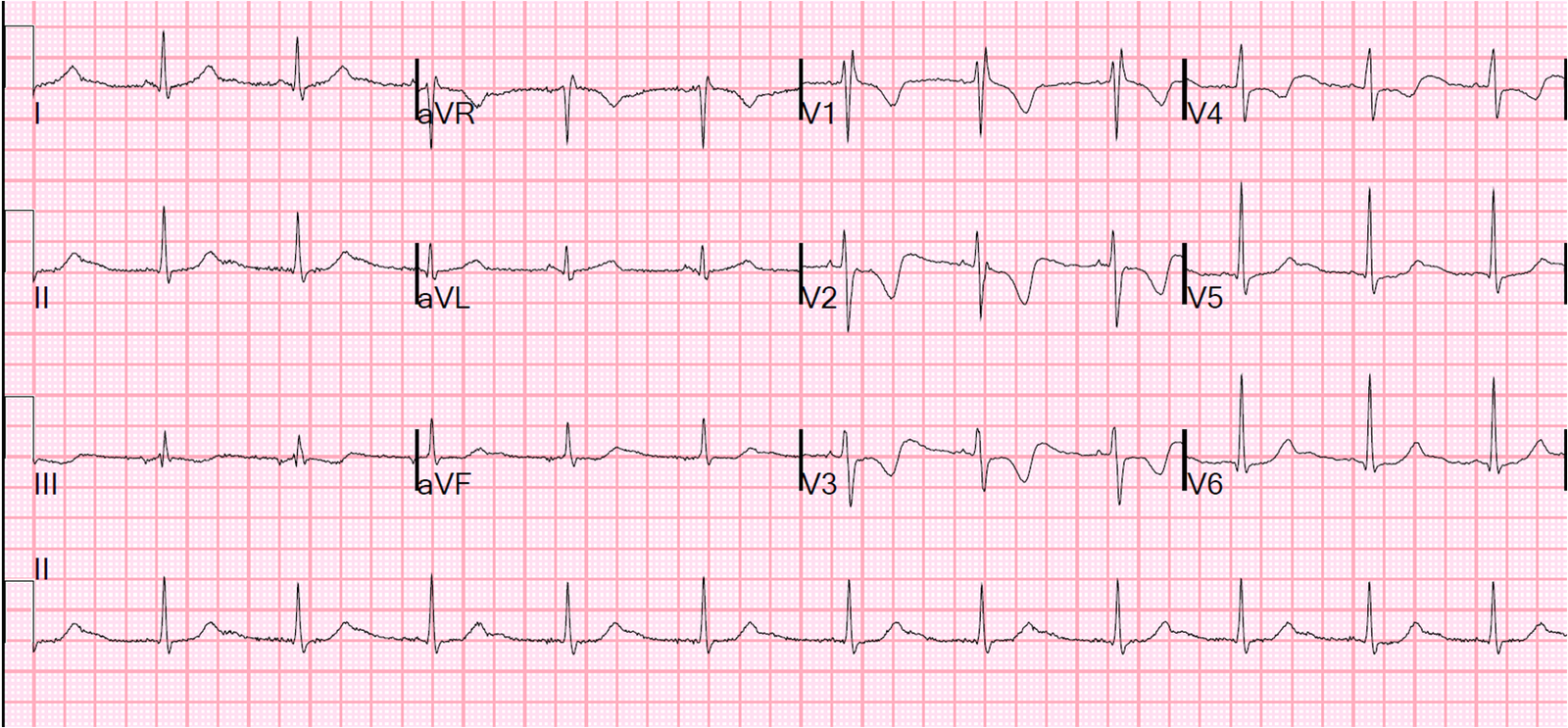
You can clearly see the peak of the T-wave in lead II across the bottom. So let’s find where the peak is on other leads:
 |
| There is sinus rhythm with inverted P-waves (low atrial pacemaker, of no clinical significance). The blue line shows the peak of the T-wave in II. Drawn up to V1-V3, you can see that the large wave is AFTER the T-wave. It is thus a U-wave, not a T-wave, and the QT is not long. The arrows point to U-waves in other leads |
The patient had a previous ECG:
 |
| It turns out she had had unspecified cardiac surgery in the past and had incomplete RBBB at baseline. As you can see, there were no U-waves on that previous ECG. |
Her K was 2.9 mEq/L. This is not terribly low, but can certainly result in ECG abnormalities.
She had K replaced to a level of 3.9 mEq/L. Then, 2 hours, 40 minutes later this ECG was recorded:
 |
| U-waves are still present but not as prominent. The treating physicians interpreted this as normalized back to baseline ECG; clearly this is not so. |
Why are U-waves still present?
1. She may have some other unspecified reason for U-waves
2. Recurrent hypokalemia: Her K may have dropped back down after replacement. For every 1 mEq/L of low potassium, there is a 200-400 mEq total body deficit. So K may shift to the intracellular space soon after replenishment, and the serum K may drop within hours after administration.
The syncope and the ECG are probably completely unrelated, though it is possible that this resulted in ventricular dysrhythmias.