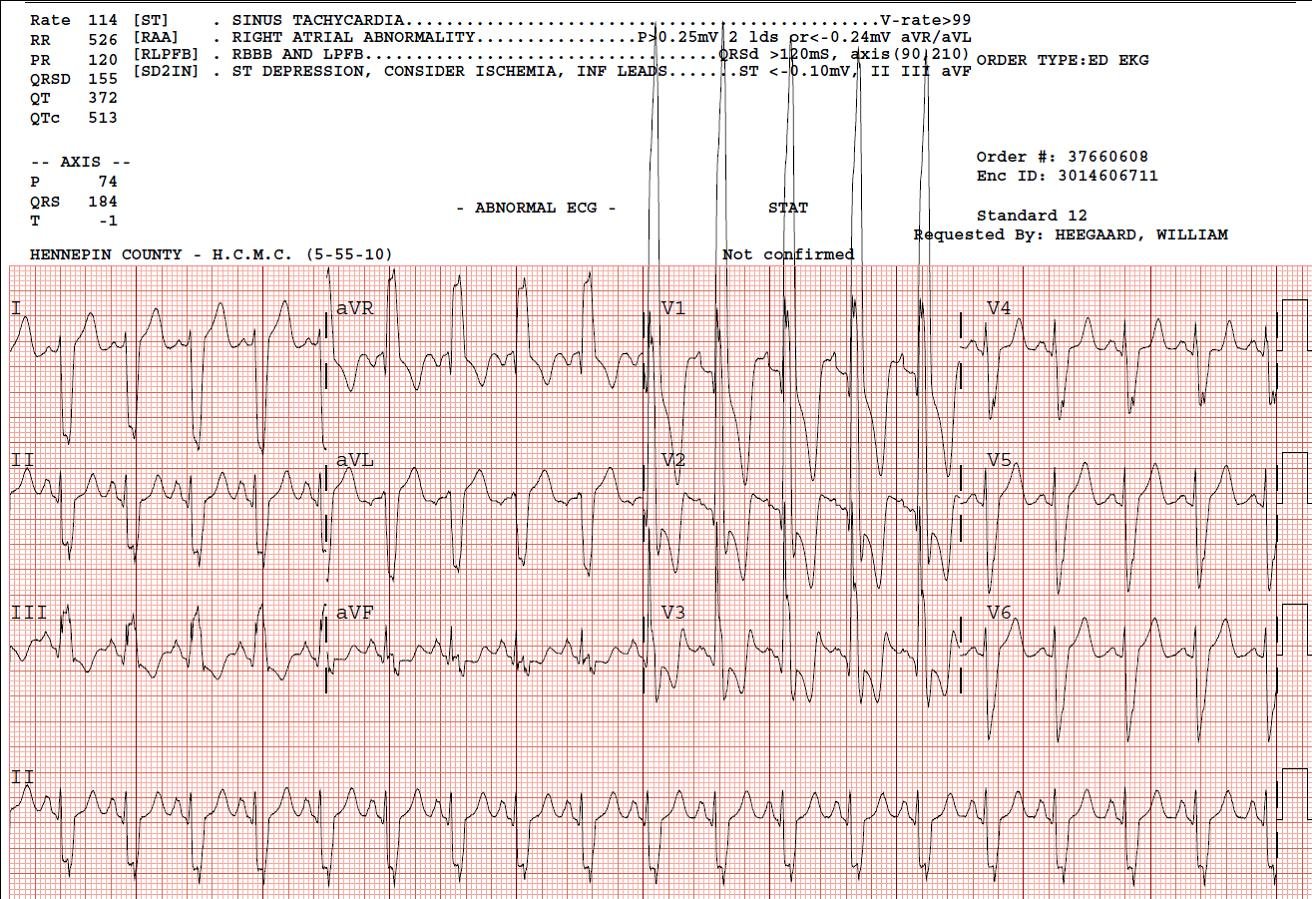
This diabetic patient with the ECG below was brought in by medics confused, tachycardic, and hyperglycemic, Kussmauling. The computerized ECG algorithm diagnosed Acute MI (I’m not sure why).
 The ECG is diagnostic of hyperkalemia, with QRS of 180 ms. The QRS improved immediately after giving 2 doses of Calcium gluconate. K returned at 7.3, with a pH of 6.91, HCO3 of less than 3. After a total of 5 doses of Ca gluconate, 6 doses of bicarb, 4 liters of fluid, and insulin, this patient with extremely severe diabetic ketoacidosis stabilized. He had some demand ischemia, with maximum troponin of 1.5, but there was no acute coronary syndrome.
The ECG is diagnostic of hyperkalemia, with QRS of 180 ms. The QRS improved immediately after giving 2 doses of Calcium gluconate. K returned at 7.3, with a pH of 6.91, HCO3 of less than 3. After a total of 5 doses of Ca gluconate, 6 doses of bicarb, 4 liters of fluid, and insulin, this patient with extremely severe diabetic ketoacidosis stabilized. He had some demand ischemia, with maximum troponin of 1.5, but there was no acute coronary syndrome.
His ECG from the next AM is shown below; the QRS is now less than 120 ms.