This case was sent by:
Maria Perez
Emergency Registrar
Monash Medical Centre
Melbourne
She obtained permission from the family to identify the location or origin of the case.
Case
This previously completely healthy 8 yo girl complained of diarrhea, vomiting, and upper abdominal pain radiating to the chest, for the past 3 days. There had been an episode of syncope 3 days prior for which she had been seen by her primary care provider, but there is no information from that visit.
Her exam was normal except for an irregular heart rate at 78, with BP of 100/60. Lungs were clear.
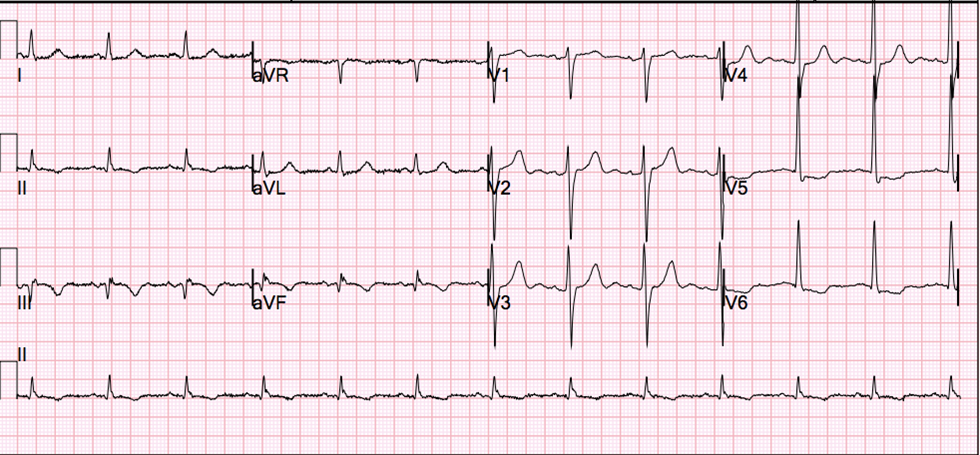
Because of the irregular heart beat and h/o syncope, an ECG was recorded:
 |
| There is an irregular rate. The image resolution is not ideal and it cannot be enlarged. All beats are supraventricular. This was my original interpretation, but was corrected (see below) by Andreas Roschl. There appear to be P-waves in front of every QRS, at a rate of about 150 (sinus tachycardia). The PR interval does not lengthen. There are some P-waves that do not conduct. Therefore, it is 2nd degree block Mobitz type II. Even more important is the presence of right bundle branch block, and probable left posterior fascicular block, with massive ST elevation. |
Correction to rhythm interpretation: sinus rhythm with short runs of PACs (i.e. atrial tachycardia).
Besides AV block, this ECG is diagnostic of injury, which in an adult would almost always be a STEMI. In a child, especially one who has viral symptoms, myocarditis is highest on the differential diagnosis.
Mobitz type II block has potential to evolve into complete (3rd degree) AV block. Unlike Mobitz type I (Wenckebach), it is associated with anterior injury (injury to the septum and bundle of HIS).
Mobitz II block in STEMI and with new BBB is a class I indication for transvenous pacing, as it frequently progresses to complete AV block.
The patient had no family history of sudden death and no recent overseas travel.
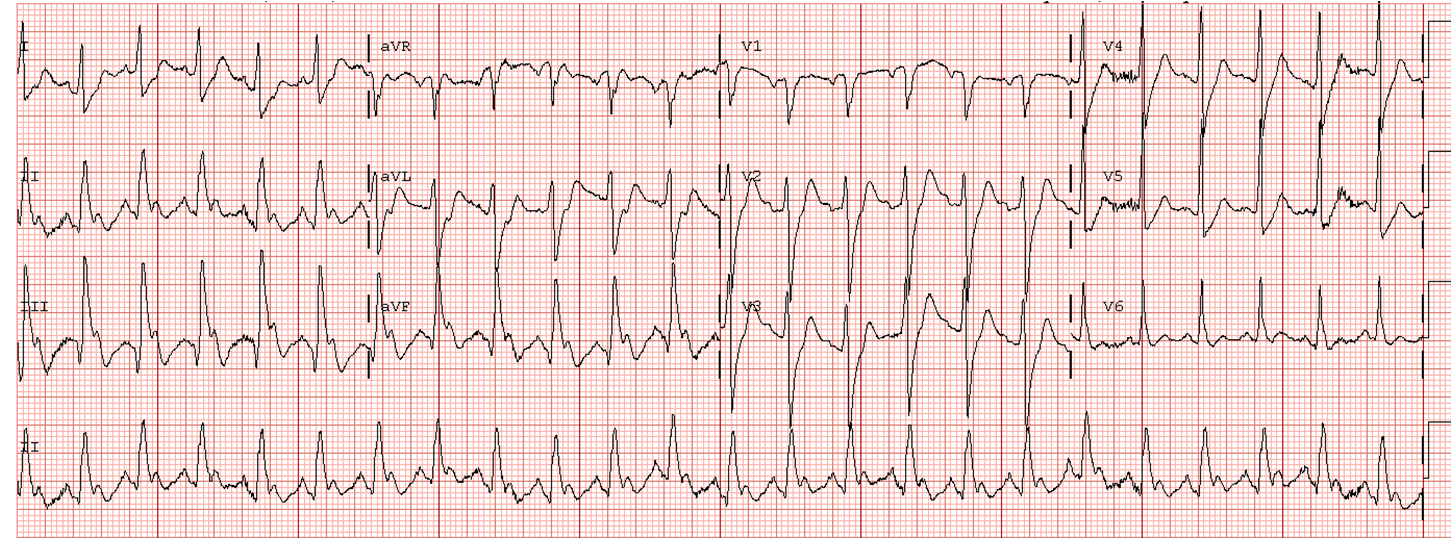
3 more ECGs were recorded before the patient could be transferred:
 |
| There is continued Mobitz II block, variably blocked. Sinus rate remains about 150. |
 |
| Continued Mobitz type II block, now with a regular 2:1 AV block. RBBB and LPFB are still present. Injury pattern continues. |
Correction to rhythm interpretation by Andreas Roschl: What appear to be P-waves without conduction may, in fact, be T-waves. This is uncertain.
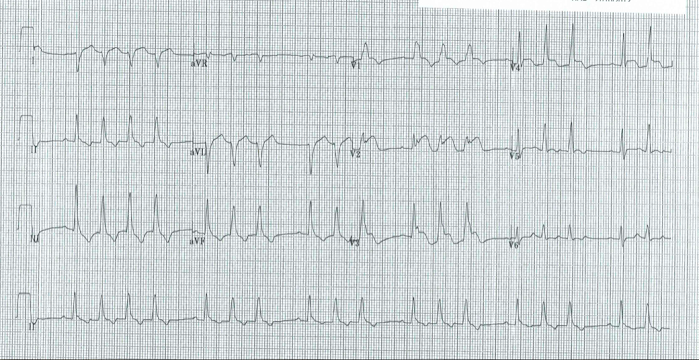
 |
| Continued Mobitz type II block, still with a regular 2:1 AV block. RBBB, LPFB, and injury continue. |
The initial troponin I was 13 ng/mL
She then had further decrease in level of consciousness en route to the referral hospital, with episodes of 3rd degree heart block with ventricular escape. She underwent transvenous pacing and was started on isoprenaline (isoproterenol).
–Immediate angiography revealed normal coronary arteries.
–Biopsy confirmed myocarditis.
–All viral PCR tests were negative.
–Echocardiogram showed severely reduced biventricular function with a septal wall motion abnormality and a small effusion.
Final diagnosis: Myocarditis, likely viral, however results non conclusive for any specific viral cause.
The last ECHO before discharge: mild-moderate concentric LV hypertrophy, good biventricular contractility, globally reduced LV myocardial velocities, normal conventional diastolic function.
She was discharged on lisinopril.
Lessons:
1. Do not hesitate to obtain an ECG in children who have any chest pain or irregular heart beat
2. Myocarditis can mimic STEMI
3. Any AV block in the presence of injury or in the presence of bifascicular block is a warning of impending complete AV block.
4. Mobitz type II block is particularly worrisome