This was contributed by an ECG enthusiast who wishes to remain anonymous.
LVH is a well-described “mimic” of STEMI. However, a diagnosis of LVH does not exclude an acute coronary occlusion, and the clinical context, including symptoms and old ECGs, must be taken into account.
A 50 year-old woman came to the ED with recent-onset chest pain.:
She
had a history of hypertension, as well as concentric LVH on a very
recent echo. Furthermore, she had markedly elevated systolic BP > 200 mm Hg.
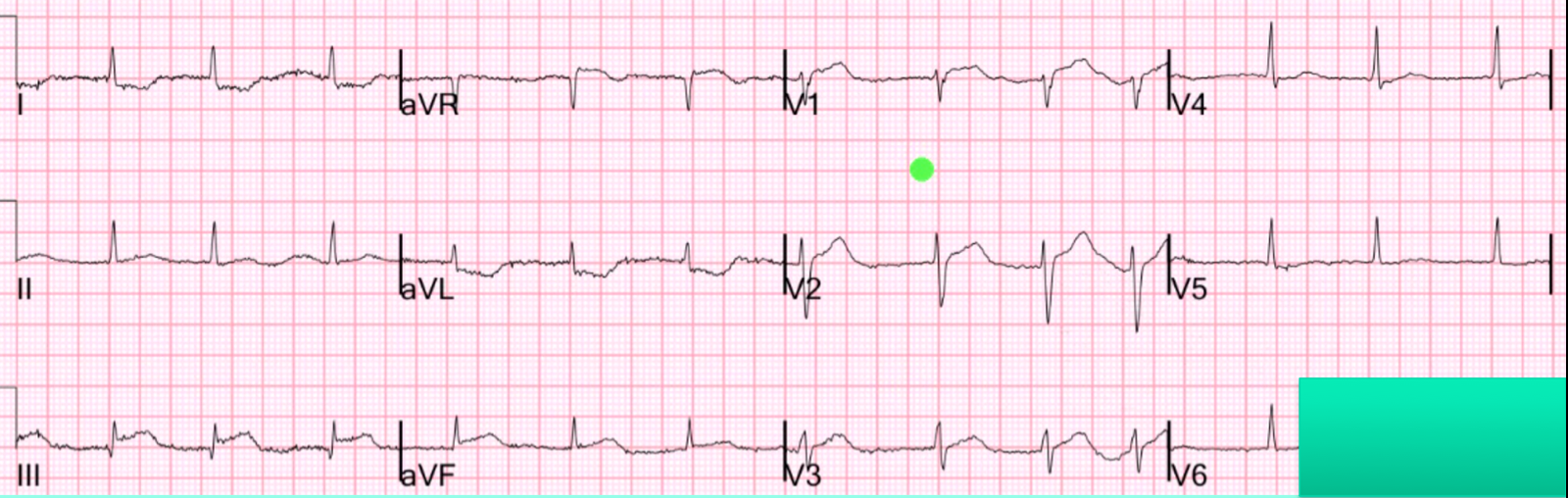
Her initial ECG:
 |
| There is STE in lead III, < 1 mm, as well as STD with inverted T waves in leads I and aVL. This pattern of STE and STD could represent an early or subtle inferior coronary occlusion. However, the R wave in aVL is ≥ 11 mm, basically diagnostic for LVH. |
Smith comment: the voltage only barely meets LVH criteria, but the morphology of the T-wave inversion in aVL has the “hockey stick” shape often seen in LVH. Furthermore, the inferior T-waves are not as large as one would suspect with a coronary occlusion (see example at bottom). I would agree with the contributor that it does not look like the typical ST-T of subtle inferior MI. But, remember, coronary occlusion can show almost nothing on the ECG. If it can show nothing, then very subtle abnormalities could be something.
The
ECG raised concerns for inferior MI, but it was decided that the STE
and STD were due to repolarization changes of LVH. Nonetheless, a repeat
ECG was obtained 1 hour later:
 |
|
Not significantly evolved from the prior ECG. |
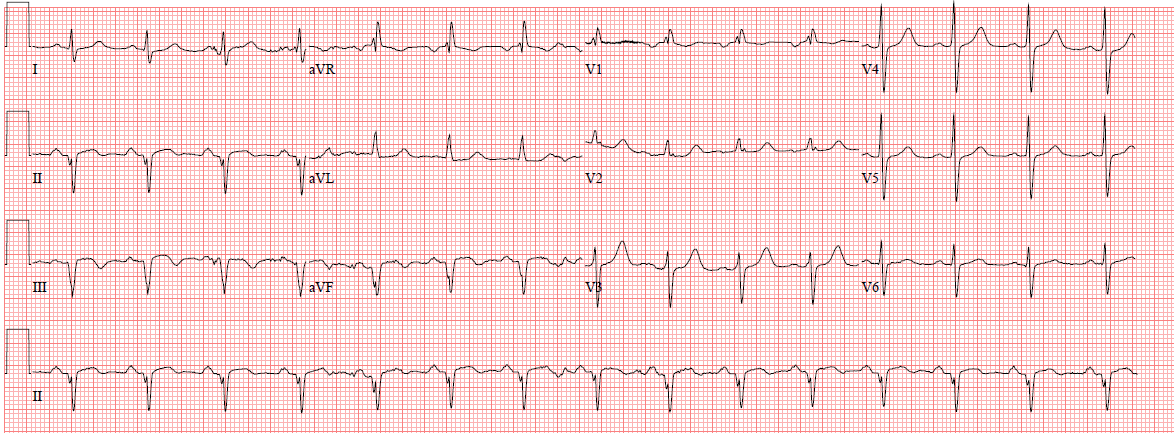
These ECGs were compared with an ECG from 1 week prior:
 |
| Although there is T wave flattening in leads I and aVL, there is no suggestion of LVH on this ECG. In fact, the ST segments in I and aVL are slightly elevated, and those in the inferior leads II and aVF subtly depressed. |
Smith comment: The change from one month ago is diagnostic of ischemia.
I very much doubt that LVH on the ECG, with ST-T repolarization abnormalities, can develop over one month. Serial ECGs are very helpful, but frequently show no or minimal evolution over one hour. One need only see this recent case I posted for another example of absence of evolution.
Contributor continued:
Given
the previously documented LVH on echo, as well as the lack of evolution over 1
hour, the new ECG changes were attributed to a combination of acute
hypertension, LVH, and different patient and limb-lead positioning. The
patient received aspirin, morphine, and nitroglycerin. The first
troponin was below the 99% cut off, and she was admitted to telemetry
for serial troponins.
Smith comment: I think it would have been appropriate to dial up the Nitro until the BP is normal, then repeat the ECG. If the ST segment abnormalities remain, then either angiography or emergency formal echo is indicated. If they resolve, then perhaps the findings are due to the severe hypertension. That is exactly what happened in this really interesting case.
Contributer continued:
Wait, why did she have an ECG from a week ago?
She
had been admitted earlier in the month for an NSTEMI without ECG
changes. On angiography, a drug-eluting stent was used to open a total
RCA occlusion. (The ECG above was post-PCI.) With
this knowledge that she had received PCI to the coronary region of
concern on the ECG (the RCA typically supplies the inferior wall) only
weeks ago, the plan was made to manage her ongoing pain medically, and
she was admitted to a telemetry bed.
ECGs were repeated at 5 hours post-arrival:
 |
| Although the R wave in aVL is still diagnostic for LVH, the STD/TWI in leads I and aVL have resolved, as has the STE in III and aVF. This proves that they were due to ACS, not LVH. |
And 6 hours post-arrival:
 |
| The R wave in aVL has regressed to her baseline height, while T wave inversions in III and aVF suggest spontaneous reperfusion of the inferior wall. |
The 8-hour troponin returned at 6.7 ng/mL. (Smith comment: we don’t know the peak, and it is not a reliable indicator of infarct size as it depends on reperfusion, which makes it rise high and quickly, infarct size, collateral circulation, and assay. However, this certainly is consistent with an acute coronary occlusion, although her ECGs
did not meet criteria for STEMI). She went to angiogram the next day and the RCA was indeed (persistently) occluded. The RCA territory, however, was now well supplied by left to right collaterals, so that the damage was not extensive. No PCI was done except for on two unrelated diagonals (off the LAD).
Why did she have an acute occlusion after getting stented?
Unfortunately,
after her PCI earlier in the month, she had been discharged home
without a Plavix prescription. In combination with aspirin, this
medication is essential for preventing in-stent thrombosis. Her echo,
which during her earlier admission had shown only concentric LVH, now
had an akinetic basal inferior segment. She was presumed to have had an
early in-stent thrombosis of the RCA DES due to insufficient platelet
inhibition.
Brief review: LVH and inferior STEMI
LVH is well appreciated as producing STE in leads V1-V3, mimicking anterior STEMI. However, no proven criteria permit a clear distinction between acute anterior ischemia and LVH.
This situation is even less clear for inferior STE when LVH criteria are met. A recent review of LVH and STEMI
highlights that “there is confusion whether the exclusion of STE
thresholds in patients with LVH is limited to leads V2-V3 or applies to
all leads.”
On the one hand…
On the one hand, LVH frequently manifests ST changes that mimic inferior STEMI.
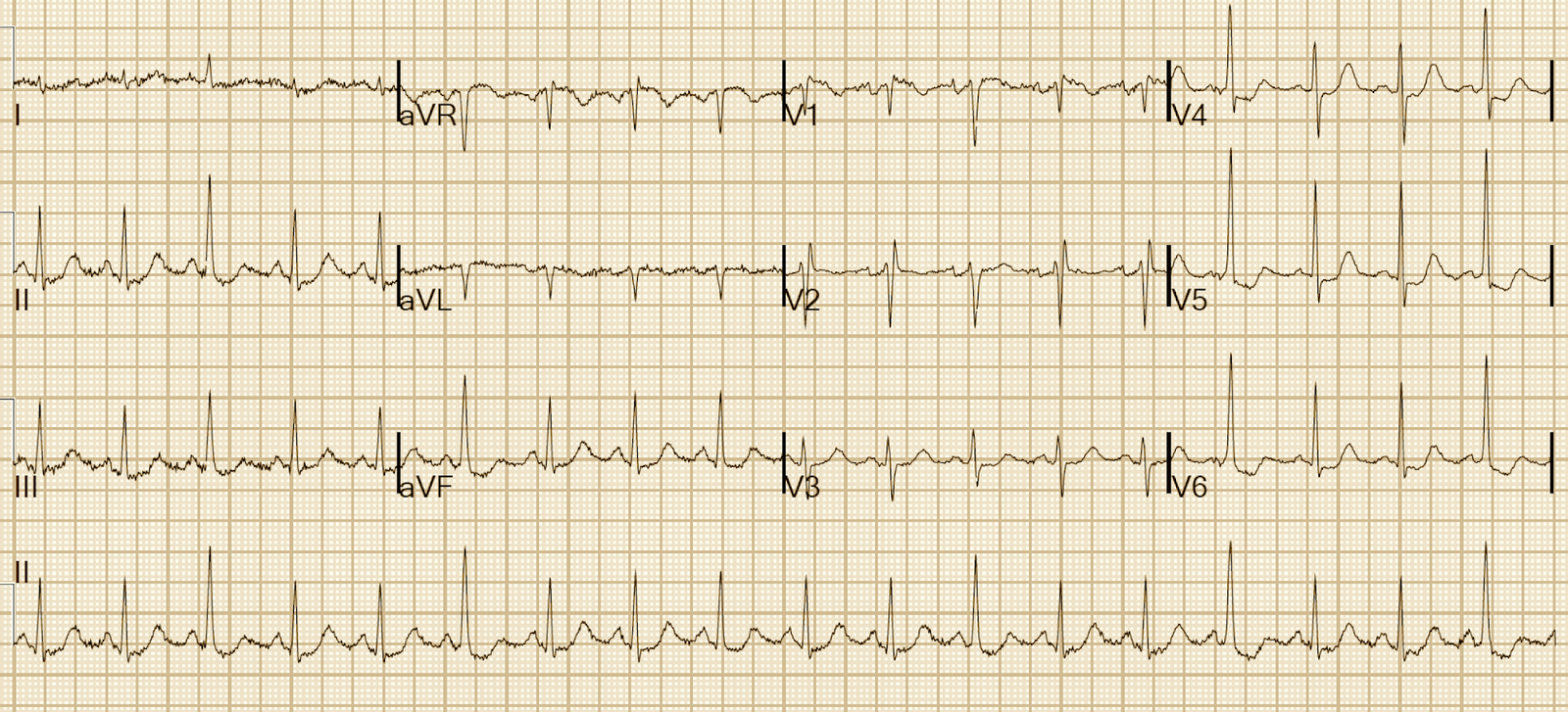
For example:
 |
| Example 2 from Life in the Fast Lane:http://lifeinthefastlane.com/ |
 |
| Case 4 from this post on Dr. Smith’s ECG blog: http://hqmeded-ecg.blogspot. |
 |
|
Case 6 from this post on Dr. Smith’s ECG Blog: http://hqmeded-ecg.blogspot. |
On the other hand…
On
the other hand, these clear examples of LVH easily met precordial-lead
criteria for LVH, as well as limb-lead criteria. Our patient, however, only met limb-lead criteria, and just barely.
Furthermore,
it is plausible that the change in axis was because the limb-lead
electrodes had been placed differently (e.g. on chest instead of arms)
than the prior ECG, or the patient positioned differently (e.g. seated
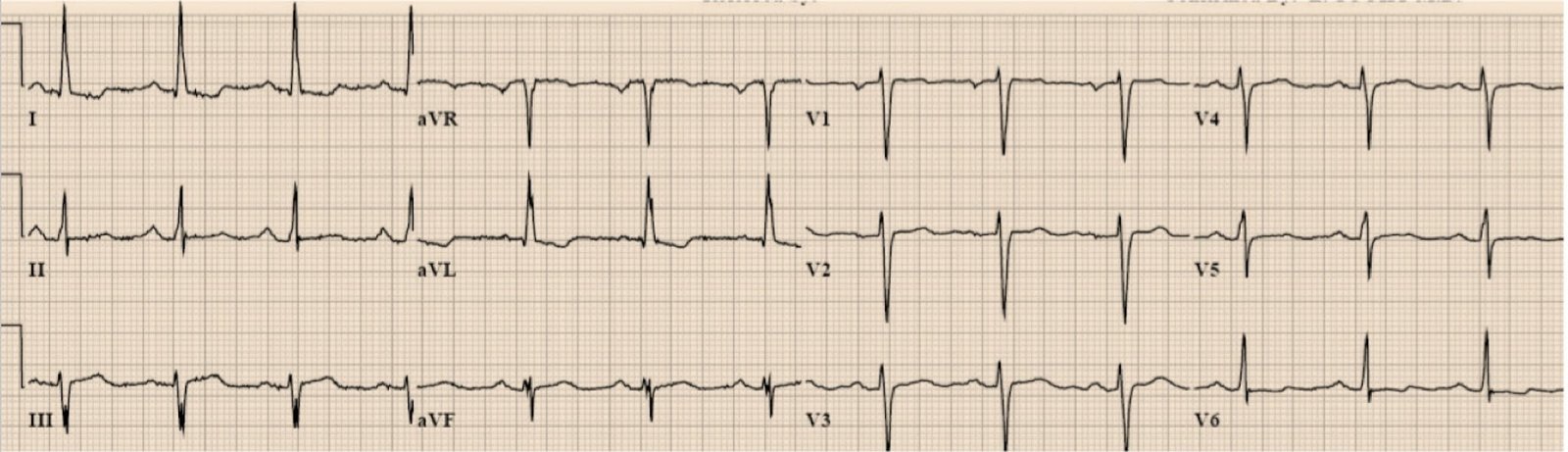
versus supine). However, such changes would not produce the ST changes we see, especially over so short a period of time. Dr Smith has a great case that also demonstrates the peril of attributing new inferior ST changes to LVH. A patient with chest pain had this ECG:
 |
| It meets criteria for LVH based on aVL, but the ST-T are far out of proportion to the QRS amplitude. This was diagnosed as MI by the emergency physician, but the interventionalist would not take the patient to the cath lab because he was convinced it was due to LVH. Furthermore, there was a previous ECG for comparison: |
 |
| Again, the previous ECG makes the diagnosis definite |