A Middle-aged male presented with chest pain of 3 hours duration. He has a history of hyperlipidemia only. There is pressure to mid-chest, radiating to the right arm, associated with diaphoresis. He never had this before. It was not related to eating. There was no cough or fever, nor trauma. There was no recent surgery, and no h/o thromboembolism.
Exam and BP were normal.
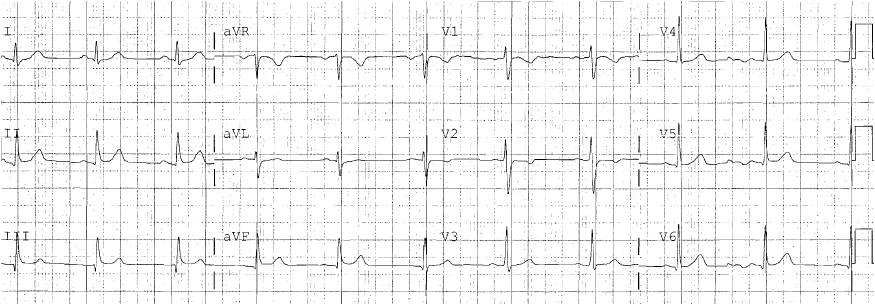
Here is the first ECG: 0526
 |
| There is ST elevation in V1-V4, with concave ST segments. Is it ischemic, or is it early repol? It does not meet STEMI “criteria,” but we know they are insensitive First, look for any reciprocal ST depression and you see it in lead III, plus some subtle STD in II and aVF. There is a bit of ST elevation in I and aVL as well. When there is reciprocal ST depression, it is likely to be LAD occlusion and the LAD occlusion formula may be falsely negative. Indeed, if you do make the calculation, with STE60V3 = 4, QTc was 385, and R-wave amplitude in V4 = 20 results in 20.98, which is quite low |
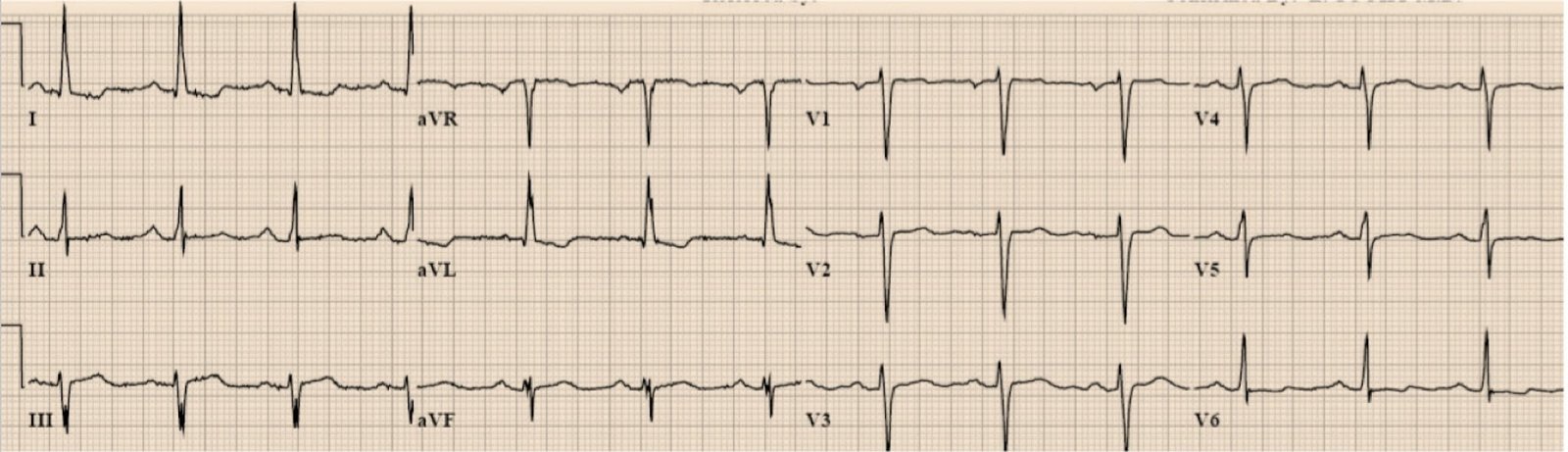
There was a previous ECG for comparison:
 |
| This is truly normal, without any significant ST elevation
You can see that the T-wave are now much larger than on the previous ECG. |
But the clinicians were not convinced.
So they did a bedside echo. Here are 3 parasternal short axis views:
They read the echo as normal, without a wall motion abnormality.
Is it normal?
Comment: I think I see a clear wall motion abnormality of the anterior wall (closest to the transducer), but wall motion abnormalities are hard to see, especially for the non-expert, and especially without contrast or stress echocardiography (speckle tracking — see these cases).
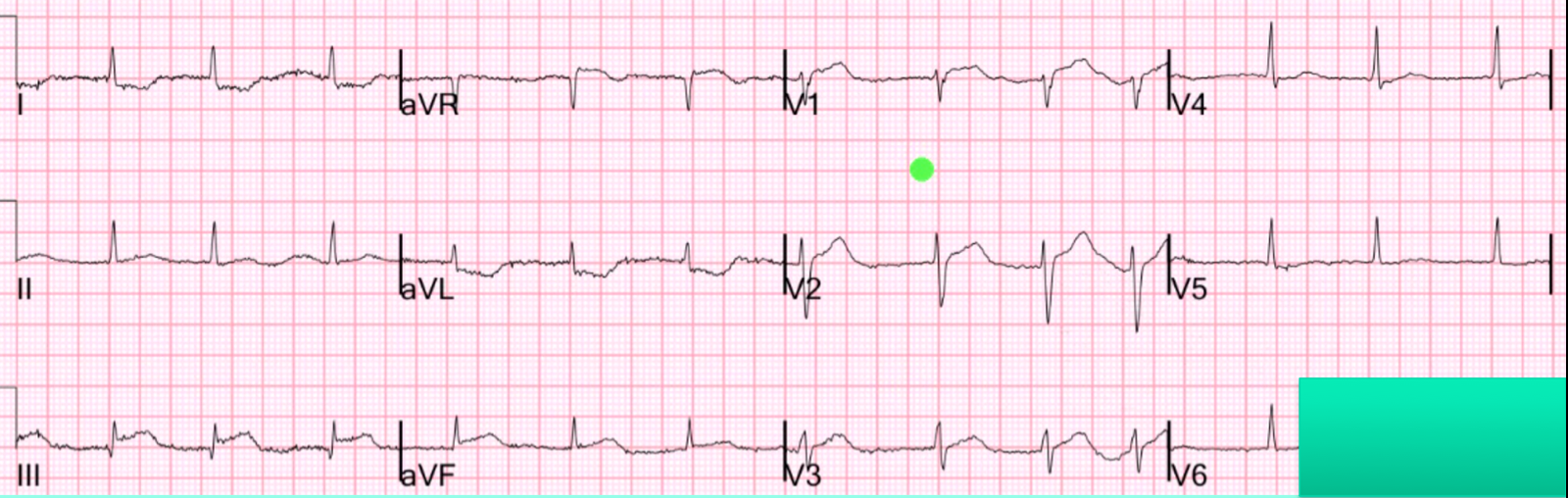
And then a repeat ECG at 0540
 |
| Not much different. |
They proceeded to look for other pathology with ultrasound:
A bedside ultrasound showed a normal aortic root and distal aorta. The gall bladder had no stones and a normal duct. There was no abdominal free fluid and no hydronephrosis. Chest X-ray showed no infiltrate and a normal mediastinum. D Dimer was normal, and lipase was minimally elevated.
Cardiology was consulted by our Pathway B, and Nitroglycerine (NTG) initiated with a plan to maximize it to eliminate pain.
Another ECG was recorded at 0556:

Then the first troponin returned at 0.036 ng/mL (99% reference = 0.030 ng/mL).
Comment: A negative troponin does not help in acute coronary occlusion, because it may be too early to be “positive.” But a positive one in a patient with no baseline pathology (heart failure, renal failure) or reason for demand ischemia (sepsis, resp failure, etc.), but only with ischemic symptoms such as chest pain, tells you that an equivocal ECG is a positive ECG.
With a nitroglycerine dose titrated up to 60 mcg/min and a systolic BP of 90-100, the nitro could not be increased further.
The decision was made to activate the cath lab in the setting of elevated troponin, concerning ECGs, refractory typical pain, and no alternative explanation such as pericarditis or aortic dissection.
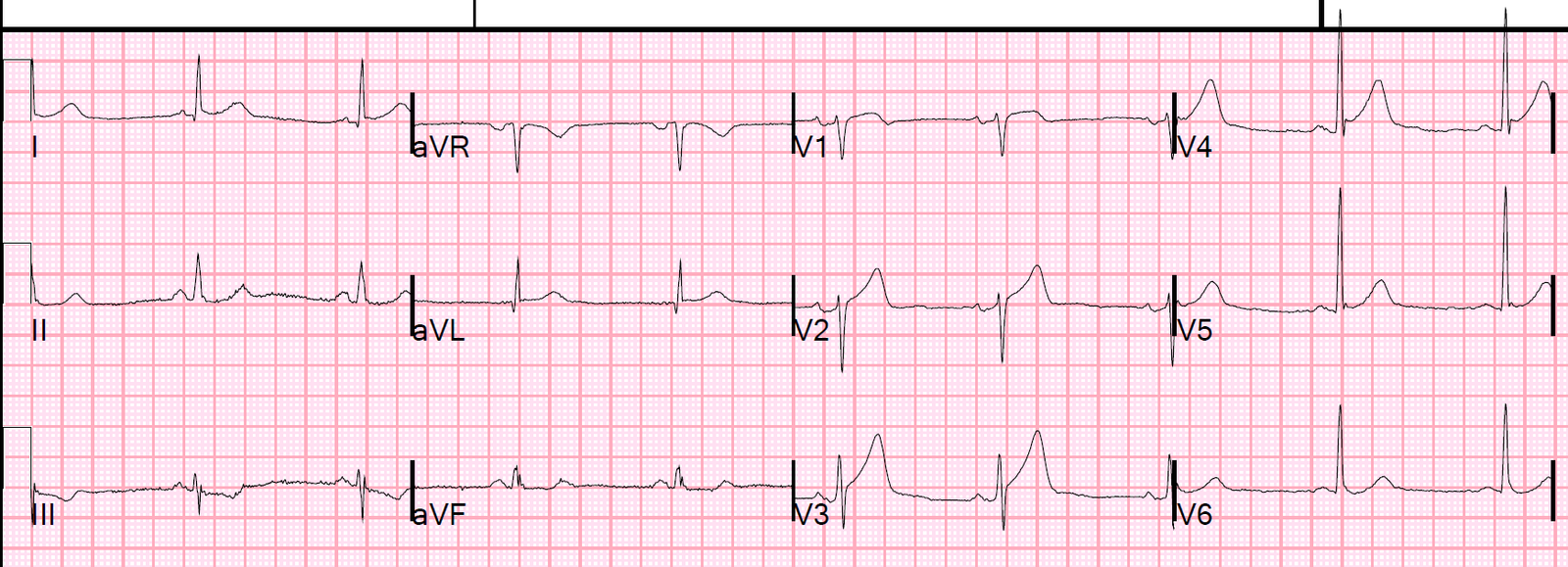
Another ECG was recorded at 0629:
 |
| Now there is more ST elevation and the change in the ECG itself is clearly diagnostic. |
0822

At angiogram, there was a 100% mid-LAD occlusion, without good collateral circulation. It was stented.
Here is the troponin profile:
 |
| Notice how the troponin suddenly rises after reperfusion and release of troponin from the cardiac circulation. The levels are quite high, consistent with a very large infarction. |
Here is the ECG the next morning:
 |
| There is still significant ST elevation, now with T-wave inversion. The persistent STE suggests that there is continued microvascular obstruction and is not a good sign. |
An echo the next day showed:
Normal left ventricular size, thickness and systolic function.
The estimated left ventricular ejection fraction is 56%.
Regional wall motion abnormality-distal septum anterior and apex
hypokinetic.
Learning Points:
1. In a patient with real suspicion of MI and anterior ST elevation that does not meet STEMI “criteria,” if there is inferior reciprocal ST depression, it is LAD occlusion until proven otherwise. This is true even if the “early repol — LAD occlusion” formula value is less than 23.4 (specific) or even if less than 22 (otherwise, a very sensitive cutpoint).
2. Compare with a previous ECG. If there is a marked change, then it is likely to be due to ACS/coronary occlusion.
Unfortunately, early repol is not completely stable: Kambara, in his longitudinal study of 65 patients with early repolarization, found that 20 patients had inferior ST elevation and none of these were without simultaneous anterior ST elevation. Elevations in inferior leads were less than 0.5mm in 18 of 20 cases. Kambara also found that, in 26% of patients, the ST elevation disappeared on follow up ECG, and that in 74% the degree of ST elevation varied on followup ECGs.
3. Bedside echo has many great uses. In suspected ACS, visualization of a wall motion abnormality may help to make the diagnosis of coronary occlusion, especially with speckle tracking; the positive predictive value is probably good. But it is hazardous to try to rule out MI with limited bedside echo. In this case, its use delayed care.
4. Finally, the clinicians did a superb job by remaining vigilant, continuing to search for alternative causes and to monitor for ACS through serial ECGs, troponin, Nitroglycerine use and more. This patient could easily have been just admitted for “rule out MI” and been left with a crippling cardiac injury.
5. Many NonSTEMI are due to coronary occlusion. Early angiography with PCI saves myocardium.