This case was sent by Laszlo Farkas, a paramedic from Hungary. He discussed it with Janos Borbas MD and Robert Sepp MD from University of Szeged 2nd
Department of Internal Medicine and Cardiology Clinic.
The case inspired me to resurrect a case that I published 10 years ago with the same ECG finding (2nd case below).
What is the finding?
What does it signify?
Case
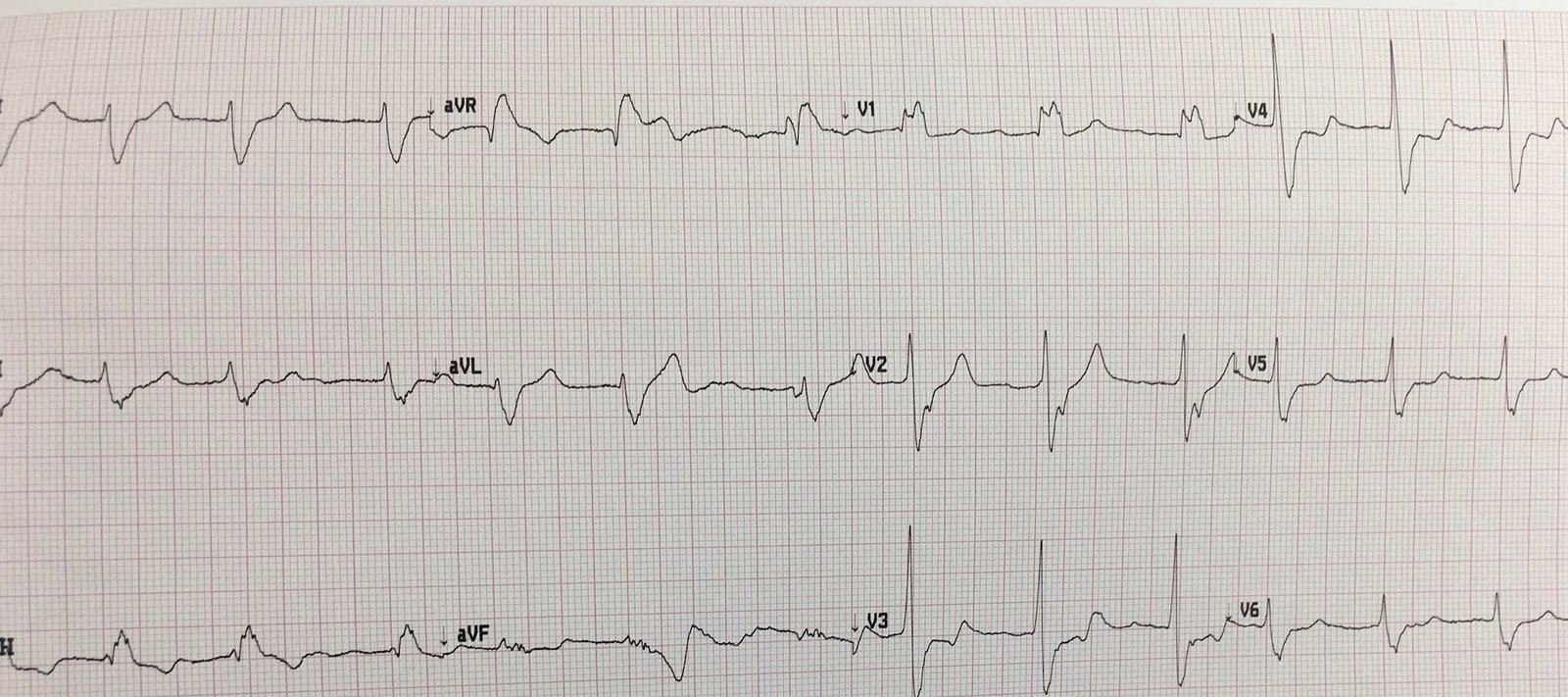
An elderly male presented with chest pain. Here is the first ED ECG:
 |
| Hint: the finding is NOT the T-wave inversion in aVL |
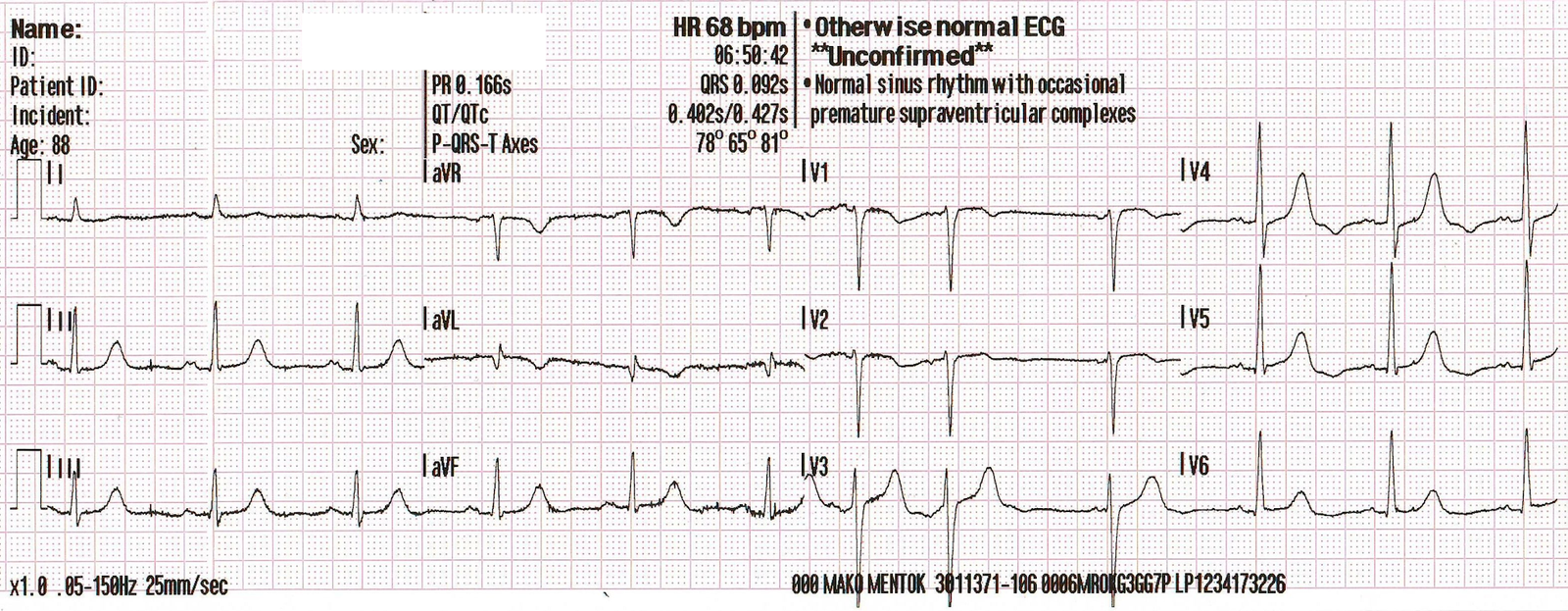
This ECG that I published 10 years ago in Critical Decisions in Emergency and Acute Care Electrocardiography has the same finding:
 |
| What is the finding? |
The finding is an inverted U-wave, as demonstrated with arrows here:
 |
| Inverted U-waves in a patient with chest pain are reported to be highly specific, but insensitive, for ischemia/infarction. |
Here is the ECG from Laszlo’s case again:
 |
| See the inverted U-waves in V3, V4, V5 |
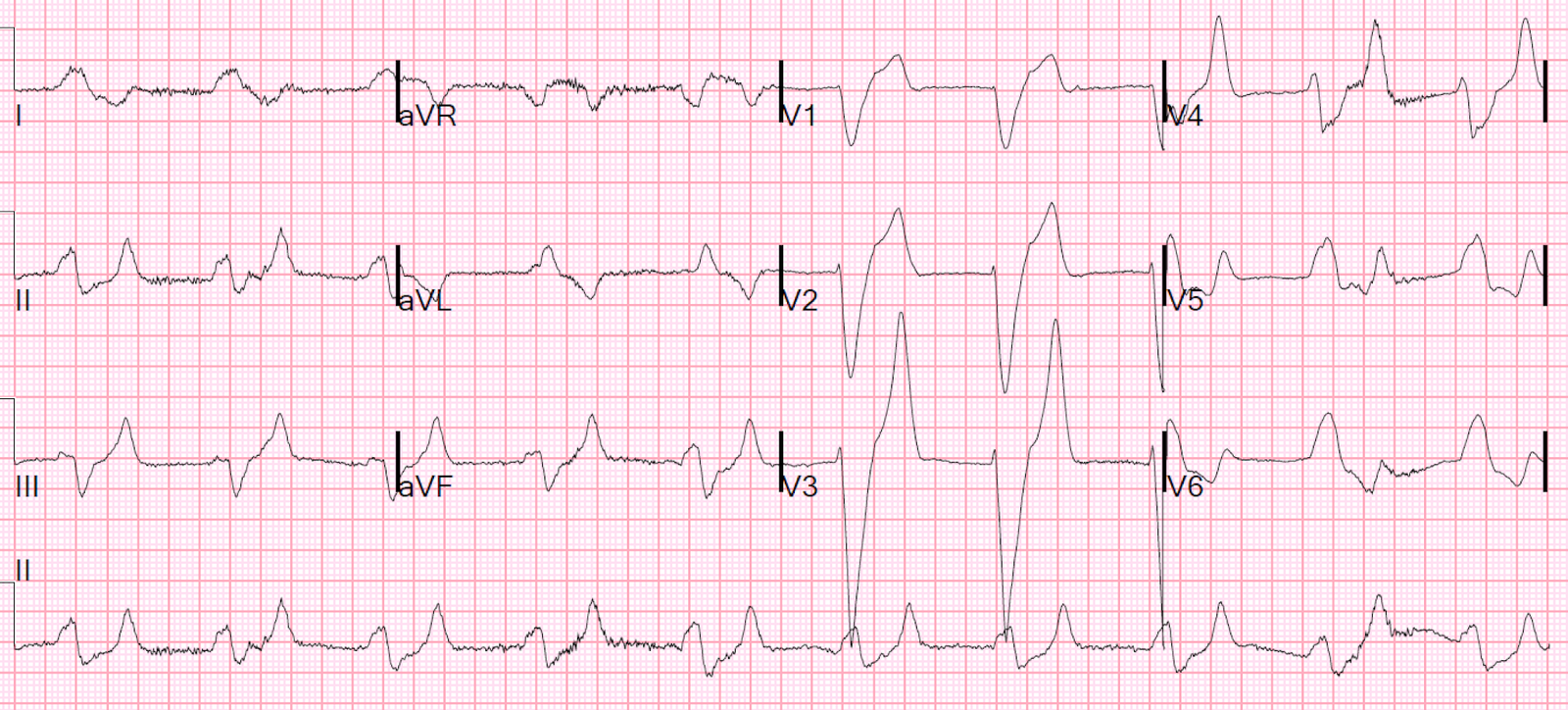
In Laszlo’s case, he recognized it and recorded another ECG 35 minutes later:
 |
| Now the U-waves are not the issue. There is obvious STEMI. |
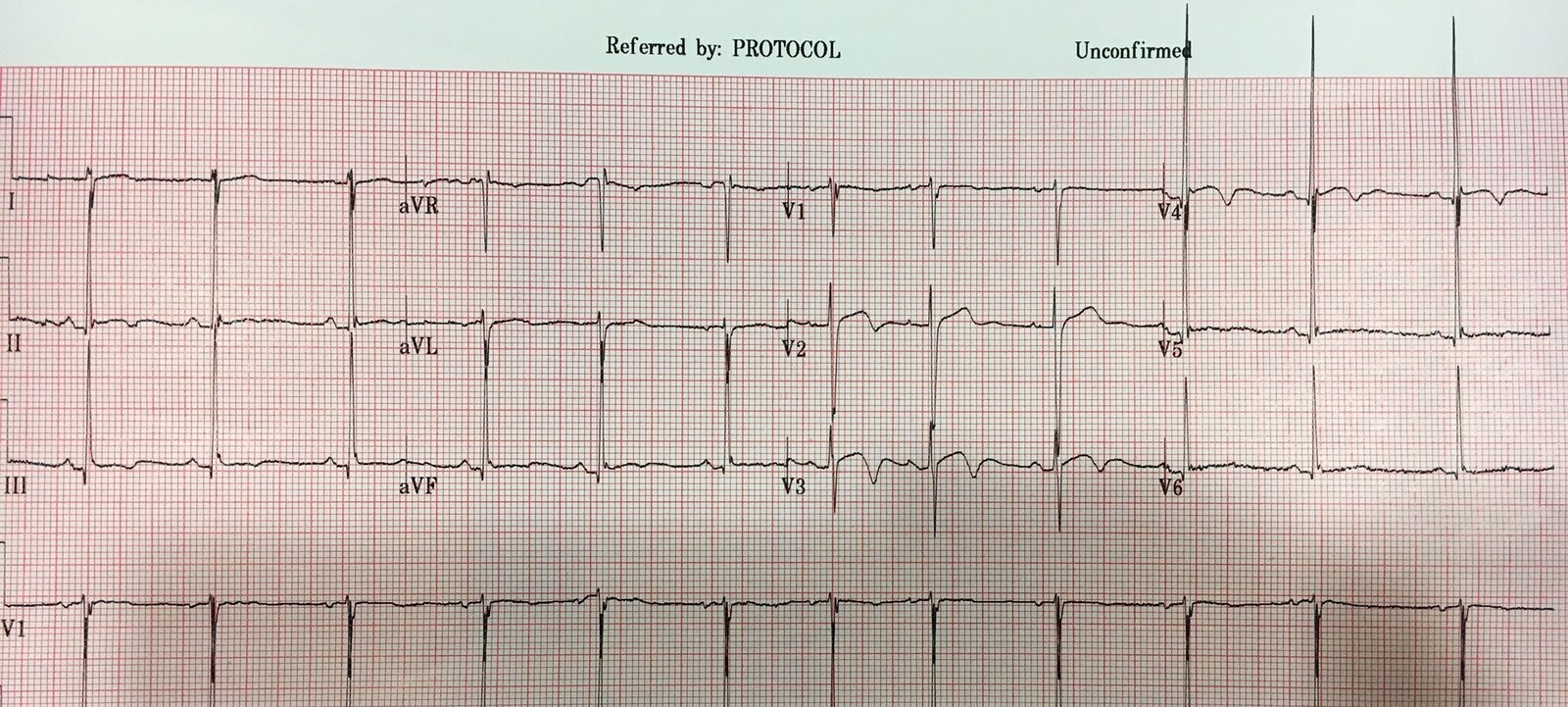
This is after reperfusion and stenting of an occluded LAD:
 |
| Terminal T-wave inversion, consistent with reperfusion. |
And then 13 minutes later:
 |
| Resolution of much of the ST Elevation (but not all).
Now U-waves are upright in V2-V550-70% reduction in STE is good evidence of tissue reperfusion |
Here is case 2:
This shows the initial ECG shown again, the comparison ECG from previous, and the reperfusion ECG after stenting of LAD that had severe subtotal thrombotic occlusion with TIMI-2 flow:
This 89 year old had an episode of unresponsiveness.

Previous ECG:

First ECG with arrows (again)
 |
| Slight STD in inferior and lateral leads, some STE in aVL, and profound negative U-waves in V3-V5. |
After Reperfusion of LAD:
 |
| Reperfusion T-waves (Wellens’ waves) |
–>