A 50-something woman with h/o hypertension and hyperaldostonism presented with severe crushing chest pain and bradycardia. EMS found the patient with a decreased level of consciousness. En route to the ED, the heart rate was 30-60 with systolic BP in the 150s and the patient was talking and answering questions.
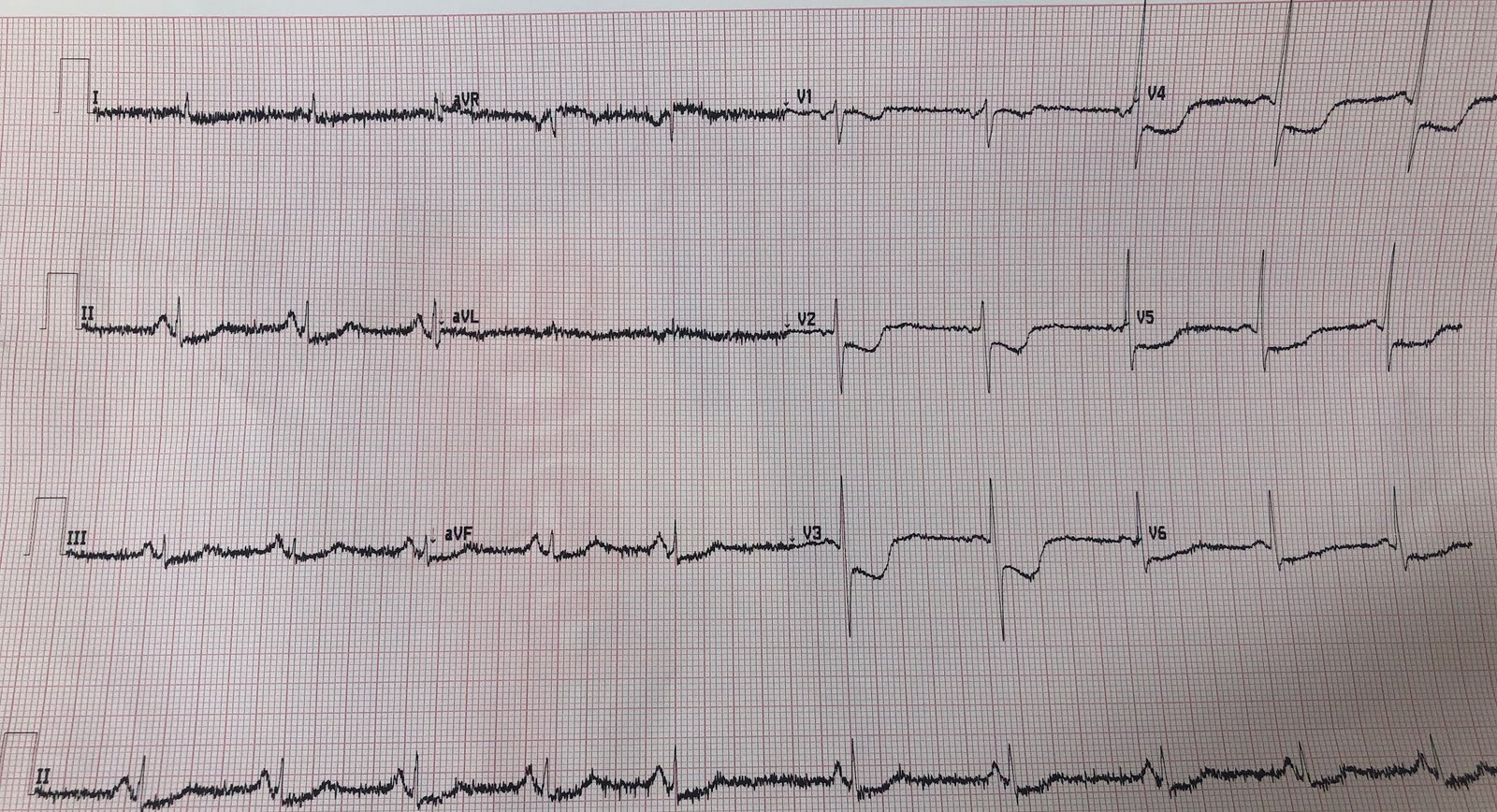
They recorded a prehospital ECG:

What do you think?
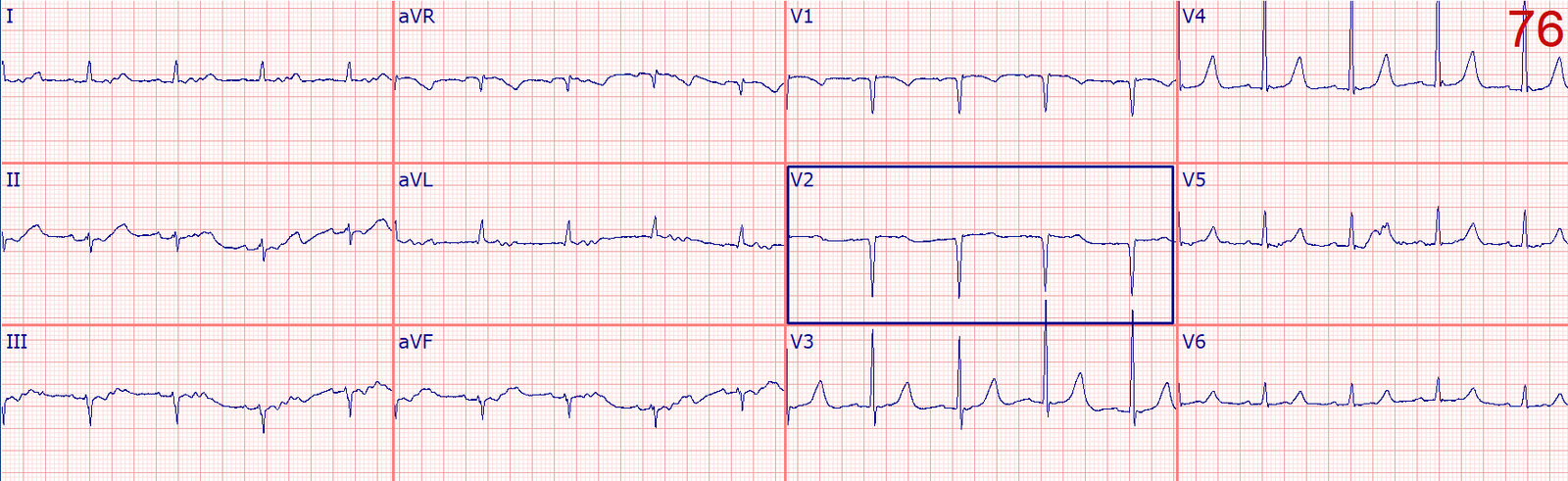
The patient arrived awake and had another ECG recorded:

What do you think?
The ED physicians correctly identified hyperkalemia and pseudoSTEMI (bradycardia, STE in V1 and V2, very peaked T-waves with a narrow bse and very flat (even downsloping) ST segment. They gave 3 g of calcium gluconate immediately. They then noted ventricular tachycardia on the monitor. The patient was unresponsive and pulseless.
After appropriate resuscitative measures and treatment for hyperkalemia, including lots of calcium, ROSC was obtained.
The K returned at 8.7 mEq/L.
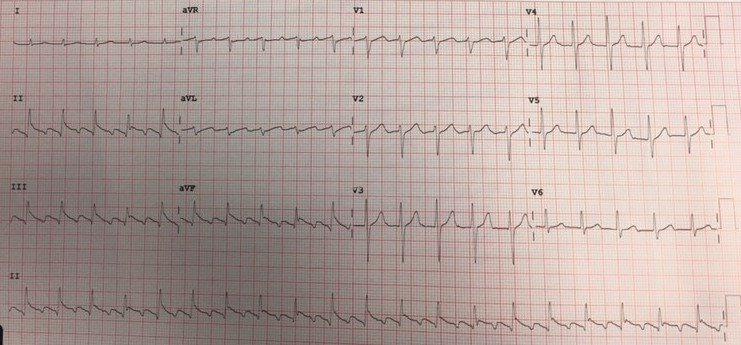
Here is the post resuscitation ECG:
Almost totally normal High Sensitivity Trop peaked at 143 ng/L (not terribly high for cardiac arrest & not high enough to support diagnosis of true STEMI as explanation for her chest pain, ST Elevation, and cardiac arrest).
Learning Point
1. Although arrest from hyperkalemia is most commonly due to widening, sine wave, and PEA, it can definitely cause VT/VF arrest.
2. Hyperkalemia causes a pseudoSTEMI pattern in V1 and V2, in addition to other well known findings.
1. Case of hyperK and VT in which I gave 15 g of calcium gluconate before the VT would stop.
Weakness, prolonged PR interval, wide complex, ventricular tachycardia
2. Case of HyperK that looks like early repol that resulted in ventricular fibrillation (see Case 3 in this post):