
The following case was incredibly interesting for other reasons, but in order to maintain confidentiality and also to allow for a subsequent case report by the physicians caring for the patient, I limit the discussion to the ECG findings and their etiology.
A man was resuscitated from an Asystolic Cardiac Arrest with Epi, bicarb, and chest compressions. He was in shock.
Here was the initial 12-lead:
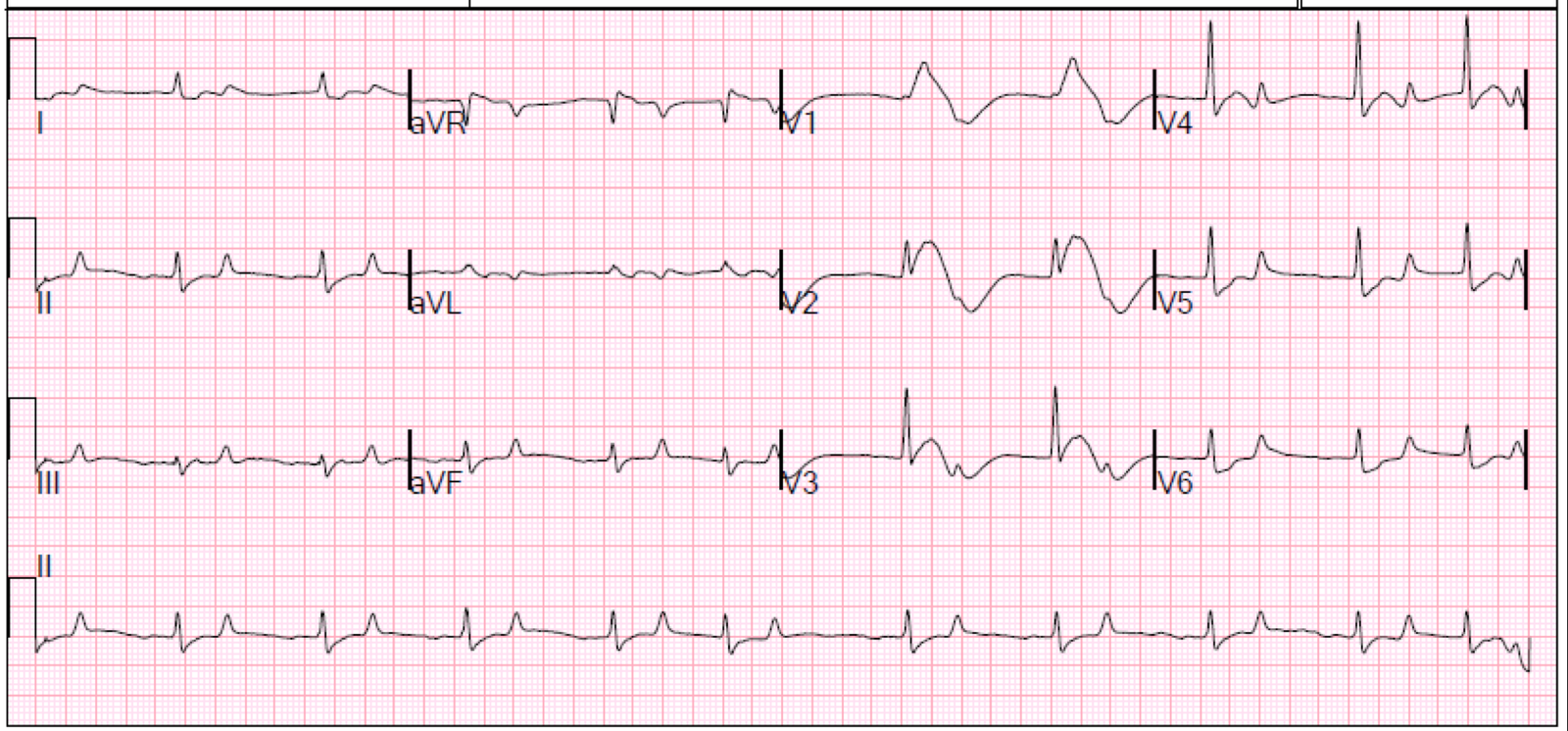 |
| This is nearly pathognomonic of at least one condition. What is it? |
There is sinus rhythm with a prolonged QRS, right precordial ST elevation, and very peaked T-waves in V4-V6. This is hyperkalemia until proven otherwise.
It is possible that the ST elevation is due to STEMI, but unlikely.
Hyperkalemia often produces a Brugada-like right precordial PseudoSTEMI pattern.
The pH was 6.65, with a K of 7.5 mEq/L.
Here are 7 other examples of PseudoSTEMI due to HyperK:
1. https://drsmithsecgblog.com/2013/06/a-tragic-case-related-to-last-post.html
2. https://drsmithsecgblog.com/2013/11/you-must-recognize-this-pattern-even-if.html
3. https://drsmithsecgblog.com/2013/06/hyperkalemia-and-st-segment-elevation.html
4. https://drsmithsecgblog.com/2013/06/this-ecg-is-pathognomonic-of-life.html
5. (there are 3 in this post): https://drsmithsecgblog.com/2013/02/right-bundle-branch-block-with-st.html
There is remarkably little literature on ECG findings in severe acidosis.
He was given Calcium, bicarbonate, and Insulin
This ECG was recorded 30 minutes after the first:
 |
| Same findings, but less pronounced, and slower rate |
The pH at this point was 6.80, with a K of 6.2 mEq/L. More Calcium and Bicarb were given.
At 1 hour, with a pH of 6.95 and K of 7.2 (difficult to control), another ECG was recorded:
 |
| Similar |
