A 30-something woman presented with CP and SOB. She was hypoxic and intubated. She had very poor LV systolic function on bedside echo. There were no B-lines and the RV was normal.
The following ECG was recorded:
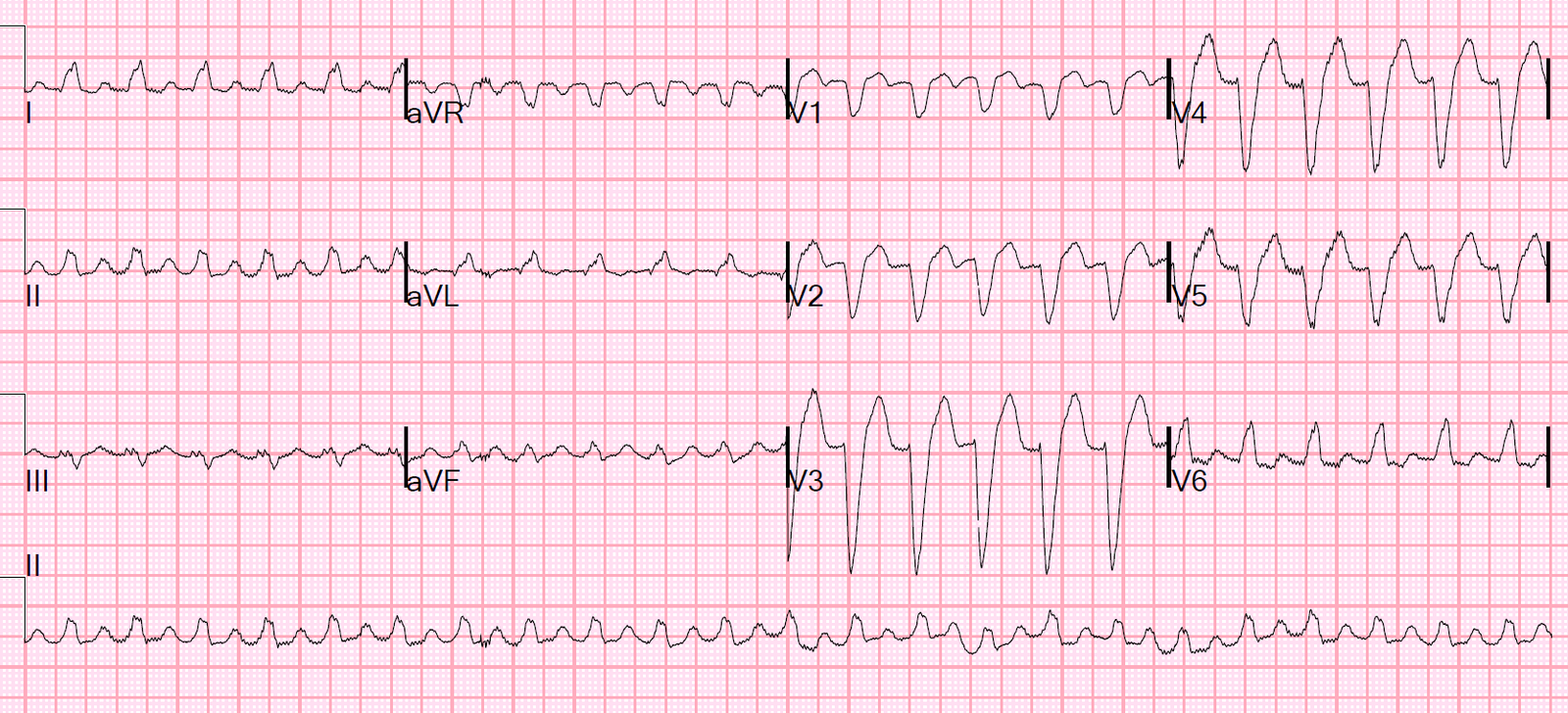 |
| Wide complex regular tachycardia at a rate of 140, no P-waves What do you think? What do you want to do? |
This ECG was texted to me on my iPhone without any clinical information, with the question: “VT or SVT with aberrancy?”
Here was my response:
“Tough one, as they always are. Looks like SVT with LBBB (LBBB morphology strongly supports SVT). Lead aVR is all negative. I am going to say SVT and I would try adenosine.”
Alternatively, it is sinus tachycardia with LBBB and P-waves are not visible. Always consider Lewis leads when this is a possibility, as they are likely to exaggerate and uncover otherwise hidden P-waves.
Further analysis, with magnification of V2 and V3:
 |
| This is typical LBBB morphology. |
When VT has its origin in the RV, it can have an LBBB-like morphology, but there are differences. Except in the case of fascicular VT, VT starts in the myocardium (not in conducting tissue) and therefore the initial part of the QRS is not rapid (it is slow). Thus, when it is VT with LBBB morphology, the onset of the LBBB-like QRS is more prolonged.
Thus, if it were VT:
1) the R-wave in right precordial leads would typically be greater than 30 ms.
Here it is about 20 ms
2) the onset of the R-wave to the nadir of the S-wave would be greater than 70 ms. In fact, it would usually be greater than 100 ms.
Here it is about 60 ms
Thus, this is very likely SVT with aberrancy (or with baseline LBBB), and the SVT is possibly sinus tachycardia with P-waves that can’t be discerned.
If the rate varies over time, sinus becomes more likely.
If it is paroxysmal SVT, Adenosine may convert it.
All ECG findings aside, severely decreased LV systolic function does make VT more likely. But these ECG findings are pretty convincing.
Case Continued
The physians thought they were dealing with ventricular tachycardia (VT)
–Cardioversion at 200 J biphasic was attempted without success.
–K was slightly low, so K and Mg were given.
–Amiodarone was given, 150 mg x 2.
–Cardioversion x 3 was apparently unsuccessful
Comment: Cardioversion would usually be effective whether SVT or VT. The question in my mind would be this: was the patient converted to sinus tachycardia (still with LBBB), at a similar rate, such that it that looked nearly identical to the SVT and the providers were unaware that the cardioversion actually worked?
–Lidocaine was given, after which patient became hypotensive.
–CXR showed pulmonary edema.
–Cardiac function on echo was very poor, prompting initiation of chest compressions.
–After 3 minutes of CPR, and 1 mg of Epi, there was ROSC with hypertension and improved cardiac function.
–The wide complex continued, but rate was down to 120, suggesting that the rhythm had indeed converted to sinus tach, but there was uncertainty as to the presence of P-waves at this point.
–A trans-esophageal echo (TEE) probe was placed by the emergency physicians in the ED. This revealed coordinated atrial followed by ventricular contraction at a rate of 120, suggesting sinus tachycardia. (Not proving it, as SVT could have atrial before ventricular contraction)
The patient remained in cardiogenic shock due to severely decreased LV systolic function. The remainder of the management is beyond the scope of this blog.
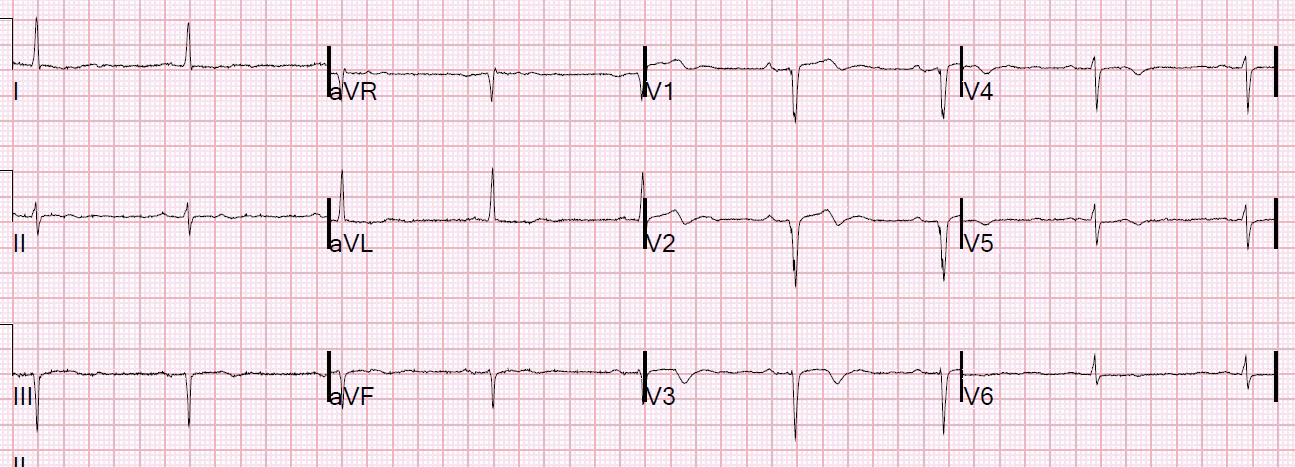
Later in the day, this ECG was recorded:
 |
| Sinus with LBBB. |
So the LBBB is definitely baseline. This is the same morphology that she had while in tachycardia, proving that the rhythm was supraventricular.
The patient recovered neurologically, but with a persistently very low ejection fraction (20%, due to new cardiomyopathy). She also had very frequent ventricular ectopy, with short runs of VT. In order to protect against dysrhythmic sudden death, she was discharged on a “Life Vest”. (2)
The diagnosis in retrospect was SVT with aberrancy in the setting of severe cardiomyopathy and acute decompensated heart failure, with later runs of ventricular tachycardia.
Learning Points:
1. If it looks just like LBBB or RBBB, it is probably supraventricular.
2. In a regular wide complex tachycardia, use adenosine if you think it is SVT. If you’re wrong and it is VT, adenosine is safe.
3. VT can have a morphology similar to LBBB, but in VT the initial part of the QRS should be prolonged, such that the septal R-wave is wider than 30 ms and/or the onset of the R- to nadir of the S-wave is greater than 70 ms.(1)
4. In a critically ill intubated patient in shock, ED transesophageal echo (TEE) can help to guide management in many ways. It can especially help to continuously monitor LV function during a resuscitation. In this case it also helped to verify sinus tachycardia.
5. A “Life Vest” (Wearable External Cardioverter Defibrillator) can be used for those who only temporarily need such a device, or as a bridge to a later implantable defibrillator (see full text article below for details, if interested).
References with links to full text