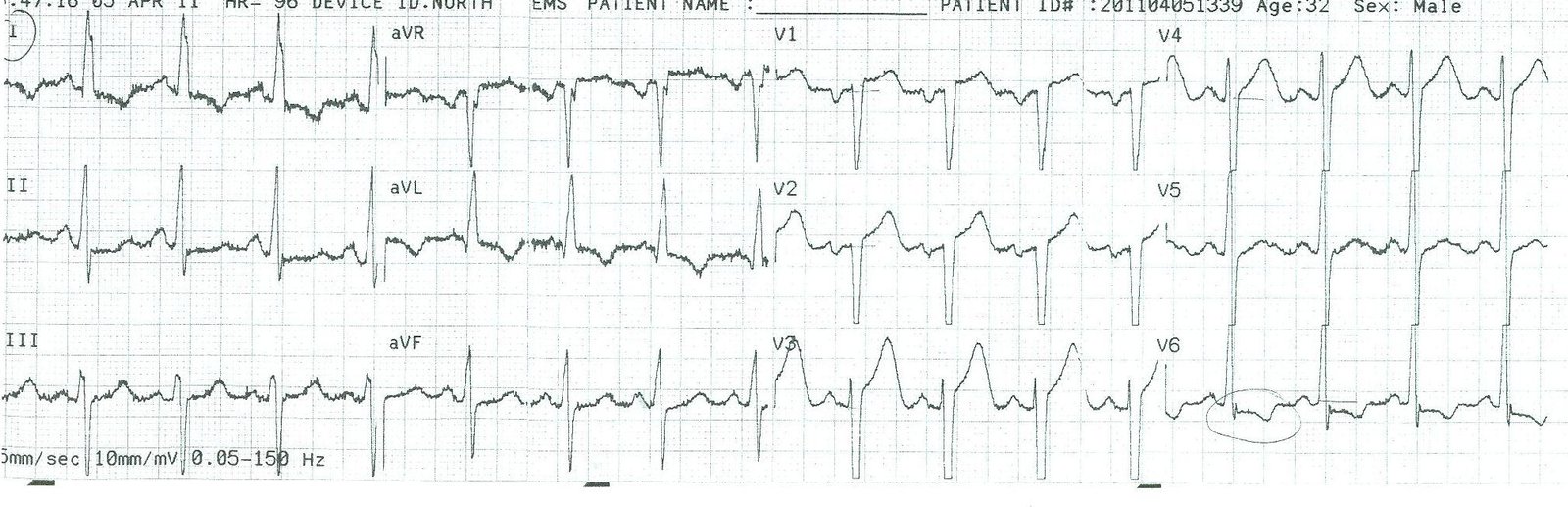
This is a 47 year old African American man with substernal and right sided chest pain, worse with inspiration. EMS was called. Prehospital EKG showed ST elevation V2 and V3 with (reportedly, tracing unavailable) some ST depression in leads II and III. The pain improved with nitro. He has a h/o smoking and hypertension. Here is his ED ECG:
 |
| There is sinus tachycardia. There is ST elevation in V1-V4, but there is also very high S-wave voltage in these leads. There is a high voltage R-wave in V5. There are no reciprocal changes. |
I was shown this ECG without the clinical info and it was clear to me that this is not STEMI because the large T-waves and ST elevation are proportional to the high voltage. Additionally, tachycardia is not common in STEMI without cardiogenic shock. AND tachycardia can exaggerate ST elevation and T-wave amplitude.
Further history: There was also a productive cough. CXR showed right sided infiltrate. In spite of all this, the cath lab was activated. Coronaries were clean.
Tachycardia was due to dehydration. Chest pain due to pneumonia. ST elevation due to LVH.
LVH is one of the most common pseudoinfarction patterns. High S-wave voltage is followed by discordant ST segments; that is, by ST elevation in precordial leads, sometimes striking.
However, LAD occlusion in these cases is very uncommon. In fact, I have only seen 2 cases of LAD occlusion in the presence of clear V1-V6 LVH. I believe, but cannot prove, that this is not because these individuals do not get LAD occlusion, but because when they do, it attenuates the voltage and erases the LVH. I am in the process of studying this.
For other cases of LVH mimicking STEMI, go here: https://drsmithsecgblog.com/search/label/LVH